Meditaliano IMAT Preparation
Lesson 18: Digestive & Excretory Systems (Complete Advanced Guide)
Introduction: Processing Nutrients and Removing Waste
This comprehensive guide covers the detailed anatomy, histology, and physiology of digestion and excretion. We will journey through the alimentary canal, explore the roles of accessory organs, and examine the intricate filtration performed by the kidneys, focusing on high-yield IMAT topics like hormonal regulation, transport mechanisms, and homeostasis.

Part 1: The Digestive System
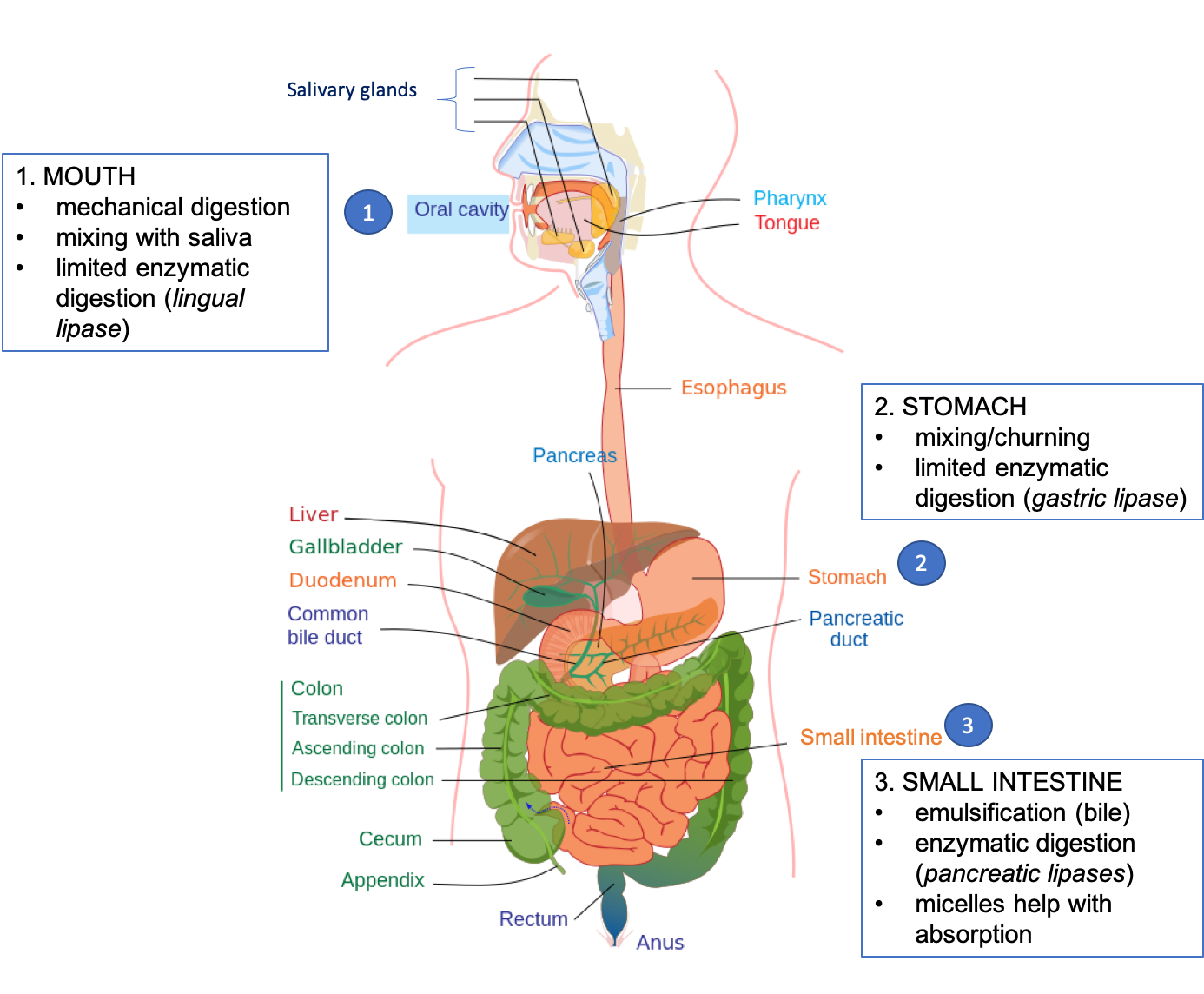
1.1 The Oral Cavity & Swallowing
Mechanical Digestion (Mastication):
- Incisors: Cutting.
- Canines: Tearing.
- Molars/Premolars: Grinding.
Chemical Digestion (Saliva): Secreted by parotid, submandibular, and sublingual glands.
- Salivary Amylase (Ptyalin): Hydrolyzes starch to maltose (pH ~7).
- Lysozyme: Antibacterial agent.
- Mucus: Lubricates food into a bolus.
Deglutition (Swallowing):
Swallowing is a complex reflex involving three phases:
- Oral Phase (Voluntary): The tongue pushes the bolus against the hard palate and moves it to the back of the throat.
- Pharyngeal Phase (Involuntary): The Epiglottis closes the trachea, the soft palate seals the nasal cavity, and breathing stops momentarily.
- Esophageal Phase (Involuntary): Peristalsis pushes the bolus toward the stomach.
Food moves down the esophagus via Peristalsis (wave-like muscle contractions of circular and longitudinal muscles).

Anatomy of the Digestive System
1.2 Stomach Histology & Function
The stomach acts as a reservoir and mixing tank (Chyme formation). The mucosa contains gastric pits composed of specialized cells:
11. Stomach Histology and Cellular Function

This diagram shows the secretory functions of Parietal cells (HCl/Intrinsic Factor), Chief cells (Pepsinogen), and G-cells (Gastrin) within the gastric glands.
- Parietal (Oxyntic) Cells: Secrete HCl (denatures proteins, activates pepsin, kills bacteria) and Intrinsic Factor (essential for Vitamin B12 absorption in the ileum).
- Chief (Peptic) Cells: Secrete Pepsinogen (inactive zymogen, activated by low pH to Pepsin).
- Goblet (Mucous) Cells: Secrete alkaline mucus to protect the lining from acid.
- G-Cells: Secrete the hormone Gastrin into the blood (stimulates acid secretion).

Simplified Gastric Pit Structure
Regulation of Gastric Secretion
Gastric juice secretion is not continuous; it occurs in three distinct phases:
- Cephalic Phase (Brain): Sight, smell, or thought of food stimulates the Vagus nerve $\rightarrow$ G-cells $\rightarrow$ Gastrin $\rightarrow$ Acid release (30% of secretion).
- Gastric Phase (Stomach): Food stretches the stomach (distension) and protein presence raises pH $\rightarrow$ Massive Gastrin release (60% of secretion).
- Intestinal Phase (Duodenum): Chyme enters duodenum. Initially stimulates, but then Enterogastric Reflex inhibits stomach via hormones (Secretin, CCK) to prevent overloading the intestine.

1.3 The Small Intestine & Accessory Organs
Divided into Duodenum (chemical digestion), Jejunum (absorption), and Ileum (B12/bile salt absorption). Features villi and microvilli to increase surface area from $0.5m^2$ to $250m^2$.
Anatomy of a Villus (Diagram)
The Villus: Specialized for absorption. Glucose/Amino acids enter blood; Fats enter the Lacteal.
Detailed Villus Structure

28. Molecular Transport at the Brush Border

This diagram shows the molecular mechanisms of efficient glucose and peptide absorption at the brush border using transporters like SGLT1 and PEPT1.
The Liver: The Chemical Factory
Blood arrives via the Hepatic Portal Vein (nutrient-rich) and Hepatic Artery (Oxygen-rich). It leaves via the Hepatic Vein.
- Bile Production: Bile salts (derived from cholesterol) emulsify lipids. Stored in Gallbladder.
- Carbohydrate Metabolism: Regulates blood glucose (Glycogenesis, Glycogenolysis, Gluconeogenesis).
- Protein Metabolism: Deamination (removing amino groups), Urea synthesis, Plasma protein synthesis (Albumin, Fibrinogen).
- Lipid Metabolism: Synthesizes lipoproteins and cholesterol.
- Detoxification: SER breaks down toxins, alcohol, and drugs.
- Storage: Vitamins A, D, E, K, B12, Iron, Glycogen.
16. Hepatic Portal System and Macro-filtration

This diagram shows how nutrient-rich blood from the digestive tract is filtered through the liver before returning to the systemic circulation via the hepatic vein.
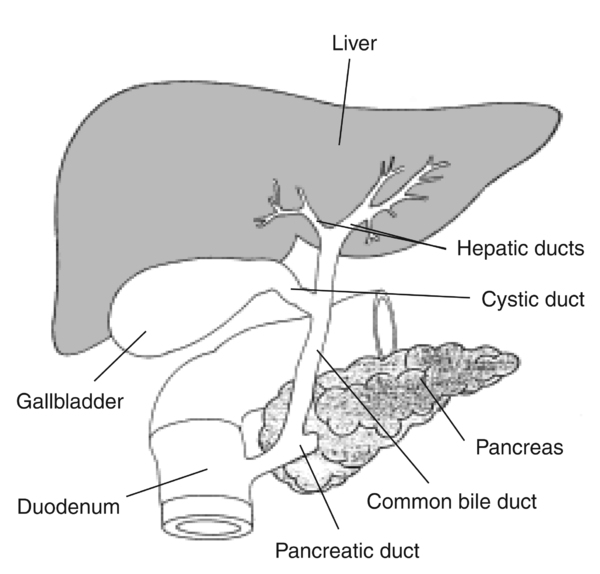
The Pancreas
- Exocrine (Acini cells): Secrete Pancreatic Juice ($HCO_3^-$ + Enzymes: Trypsin, Lipase, Amylase) into the duodenum via the pancreatic duct.
- Endocrine (Islets of Langerhans): Insulin ($\beta$-cells) and Glucagon ($\alpha$-cells) regulate blood sugar.
Proteases are secreted as inactive precursors to prevent autodigestion (eating the pancreas itself).

26. Zymogen Activation Cascade

This diagram details the complex cascade where inactive pro-enzymes from the pancreas (e.g., trypsinogen) are activated within the intestinal lumen to prevent autodigestion of the pancreas.

1.3a The Hepatic Lobule
The functional unit of the liver is the Lobule, a hexagonal structure centered around a Central Vein.
12. Liver Lobule and Microstructure

This diagram illustrates the portal triad (portal vein, hepatic artery, and bile duct), the blood flow towards the central vein, and the retrograde flow of bile within the liver lobule.

27. Sinusoids and Hepatocyte Co-transport

This diagram illustrates the exchange between liver sinusoids and hepatocytes, specifically showing bile acid secretion and sodium co-transport mechanisms that regulate the internal cellular environment.

1.4 Detailed Mechanisms of Absorption
Absorption occurs mainly in the Ileum via specific transport mechanisms:
A. Carbohydrates & Proteins (Enter Blood)
- Glucose/Galactose: Secondary Active Transport (SGLT1). Co-transport with $Na^+$. Sodium gradient is maintained by the Na+/K+ pump on the basolateral membrane.
- Fructose: Facilitated Diffusion (GLUT5).
- Amino Acids: Secondary Active Transport (Co-transport with $Na^+$).
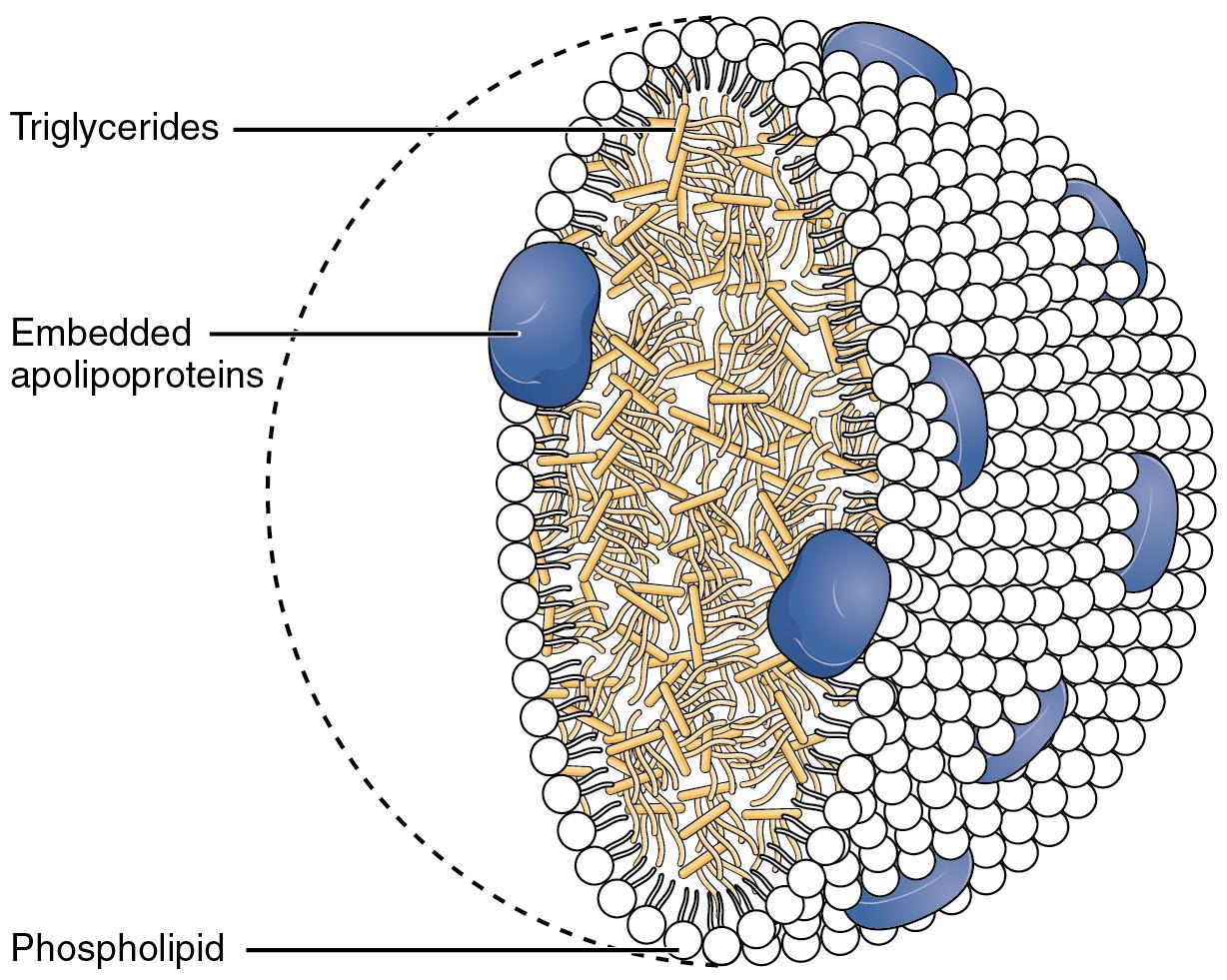
B. Lipids (Enter Lymph)
Fat absorption is complex because lipids are non-polar:
- Emulsification: Bile salts break large drops into droplets.
- Digestion: Lipase hydrolyzes Triglycerides $\rightarrow$ Fatty Acids + Monoglycerides.
- Micelle Formation: Bile salts surround fatty acids to ferry them to the epithelial surface.
- Diffusion: Fatty acids diffuse into the cell.
- Chylomicron Formation: ER resynthesizes Triglycerides and packages them with proteins (Lipoproteins).
- Exocytosis: Chylomicrons enter Lacteals (Lymphatic system), NOT blood capillaries. They eventually drain into the venous blood via the thoracic duct.
15. Lipid Digestion and Absorption

This visual guide shows the process of emulsification by bile salts, micelle formation, chylomicron synthesis within the cell, and subsequent transport into the lacteals.
17. Carbohydrate and Protein Digestion Pathway

This visual map traces the step-by-step activation of digestive enzymes from the oral cavity to the duodenum and the breakdown of macronutrients into their final absorbable products.
1.5 The Large Intestine & Gut Microbiome
The colon is not just for waste. It plays a critical role in homeostasis and immunity.
- Water Absorption: Reabsorbs ~90% of remaining water. Failure leads to diarrhea.
- Gut Flora (Microbiome): Symbiotic bacteria (e.g., E. coli, Bacteroides) synthesize Vitamin K (clotting) and B Vitamins (Folic acid).
- Fermentation: Bacteria ferment undigested carbohydrates (fiber) into short-chain fatty acids (energy for colon cells).
Broad-spectrum antibiotics can wipe out gut flora, leading to Vitamin K deficiency or opportunistic infections (e.g., C. difficile causing pseudomembranous colitis).
20. Colon Symbiosis and Defense

This diagram illustrates the role of gut microbiota in fermenting dietary fiber into short-chain fatty acids (SCFA) and maintaining the mucosal barrier and tight junctions.
Part 2: The Excretory System
Function: Homeostasis of fluids, excretion of nitrogenous waste (Urea), and Acid-Base balance.
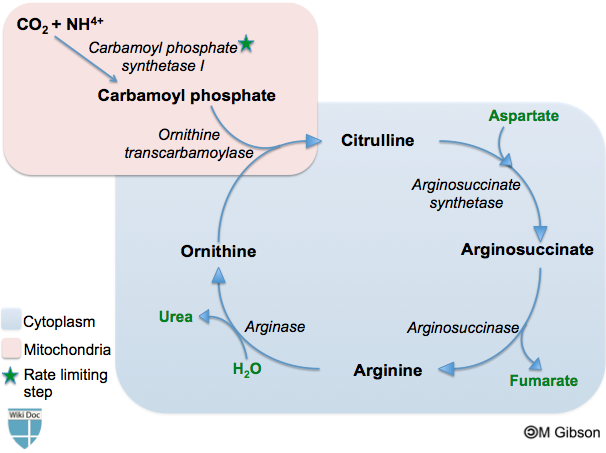
2.1 Nitrogenous Waste: The Liver's Role
Before excretion, excess amino acids must be processed in the Liver (Deamination).
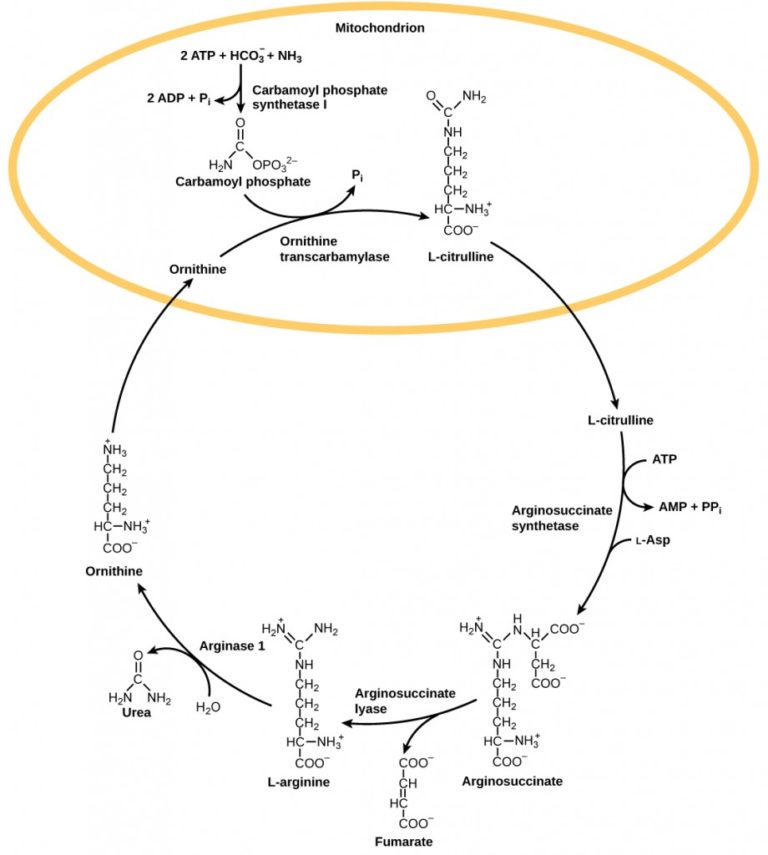
Ornithine Cycle
$$NH_3 \text{ (Toxic)} + CO_2 \longrightarrow \text{Urea (Less Toxic)} + H_2O$$Nitrogenous waste varies by animal (Ammonia=Fish, Urea=Mammals, Uric Acid=Birds/Reptiles). Urea is water-soluble and less toxic than ammonia, allowing it to be concentrated in urine.
14. Urea Cycle (Ornithine Cycle)

This flowchart details the conversion process in the liver where highly toxic ammonia is transformed into safe, water-soluble urea for excretion.
2.2 Detailed Nephron Physiology
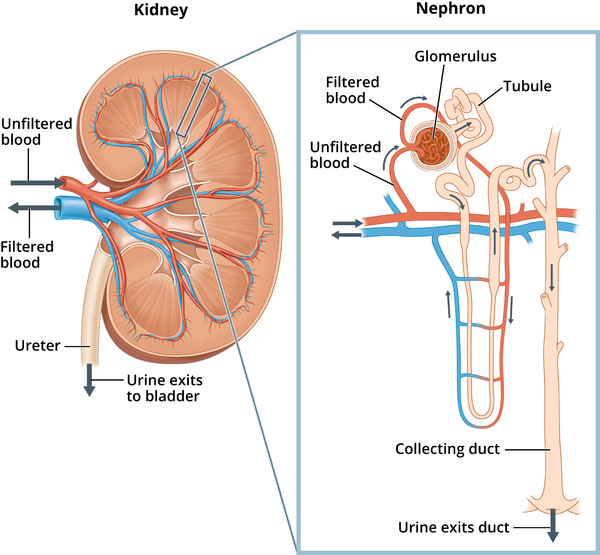
Schematic Structure of the Nephron
A. Ultrafiltration (The Barrier)
Occurs in Bowman's Capsule. Hydrostatic pressure forces fluid out. The filter has 3 layers preventing cells and proteins from entering urine:
- Fenestrated Endothelium: Capillary wall with pores.
- Podocytes: Epithelial cells with "foot processes" forming filtration slits.
Basement Membrane: Mesh of collagen and negative charge (The effective filter for proteins).
13. Glomerular Filtration Barrier

This diagram shows the three-layer molecular filter composed of fenestrated endothelium, basement membrane, and podocytes that prevents blood cells and large proteins from entering the filtrate.
Autoregulation of GFR: The kidney maintains constant filtration despite BP changes via:
- Myogenic Mechanism: Arteriole smooth muscle contracts when stretched (high BP).
- Tubuloglomerular Feedback: Macula Densa cells sense high NaCl in filtrate and constrict the afferent arteriole.

B. Selective Reabsorption (PCT)
100% of Glucose and Amino Acids are reabsorbed here, along with 65% of water and ions.
18. Proximal Tubule Cellular Reabsorption

This detailed cellular diagram shows the mechanism of 100% glucose reabsorption using SGLT1 (Sodium-Glucose Transporters) and the Na+/K+ pump on the basolateral membrane.
C. The Counter-Current Multiplier (Loop of Henle)
- Descending Limb: Permeable to water, Impermeable to salts. Water leaves. Filtrate becomes concentrated.
- Ascending Limb: Impermeable to water, Actively pumps $Na^+/K^+/Cl^-$ out. Filtrate becomes dilute.
- Result: Medulla becomes salty (Hypertonic), creating the gradient necessary for ADH to work later.

2.3 Kidney in Acid-Base Balance
The kidneys regulate blood pH (7.35-7.45) slower but more powerfully than lungs.
- Reabsorption of Bicarbonate ($HCO_3^-$): Occurs mainly in PCT. Bicarbonate acts as a buffer.
- Secretion of Hydrogen Ions ($H^+$): $H^+$ is actively secreted into the filtrate in PCT and DCT.
- Ammoniagenesis: Generation of ammonia to buffer $H^+$ in urine ($NH_3 + H^+ \rightarrow NH_4^+$).
2.4 RAAS & ADH
ADH (Vasopressin)
- Trigger: High blood osmolarity (Dehydration). Detected by hypothalamus osmoreceptors.
- Action: Inserts Aquaporins (water channels) into Collecting Duct.
- Result: Water reabsorption, Concentrated urine, Decreased osmolarity.
Aldosterone (RAAS)
- Trigger: Low Blood Pressure (detected by JGA) $\rightarrow$ Renin $\rightarrow$ Angiotensin I $\rightarrow$ Angiotensin II $\rightarrow$ Aldosterone.
- Action: Increases $Na^+$ reabsorption and $K^+$ secretion in DCT/Collecting Duct.
- Result: Water follows salt (osmosis) $\rightarrow$ Increased Blood Volume/Pressure.

19. Hormonal Regulation of the Distal Nephron

This diagram visualizes the control of urine concentration via Aldosterone (Na+ recovery) and ADH (water reabsorption) in the distal tubule and collecting duct.
The RAAS Pathway
Summary: Enzymes & Hormones
| Substance | Origin | Target/Substrate | Action |
|---|---|---|---|
| Salivary Amylase | Mouth | Starch | Starch $\rightarrow$ Maltose |
| Pepsin | Stomach (Chief) | Proteins | Proteins $\rightarrow$ Peptides |
| Trypsin | Pancreas | Proteins | Proteins $\rightarrow$ Peptides |
| Lipase | Pancreas | Lipids | Triglycerides $\rightarrow$ Fatty Acids |
| Gastrin | Stomach (G-cells) | Stomach | $\uparrow$ HCl secretion |
| Secretin | Duodenum | Pancreas | $\uparrow$ Bicarbonate release (Neutralize) |
| CCK | Duodenum | Gall Bladder | Bile release |
| Enterokinase | Duodenum | Trypsinogen | Activates Trypsinogen $\rightarrow$ Trypsin |