The Ultimate Cardiovascular System & Advanced Hemodynamics
A definitive, exhaustively detailed masterclass designed specifically for IMAT preparation. This document completely integrates the gross anatomy of the heart, structural characteristics of the pericardium and myocardium, the intrinsic conduction system, the cardiac cycle, detailed hemodynamics (Cardiac Output, Preload, Afterload, Contractility), and advanced clinical correlations including Atherosclerosis, Myocardial Infarction, and Congenital Pathologies.
100% Curriculum Coverage
Est. Reading Time: 150 mins
Part 1: Gross Anatomy and Structural Orientation
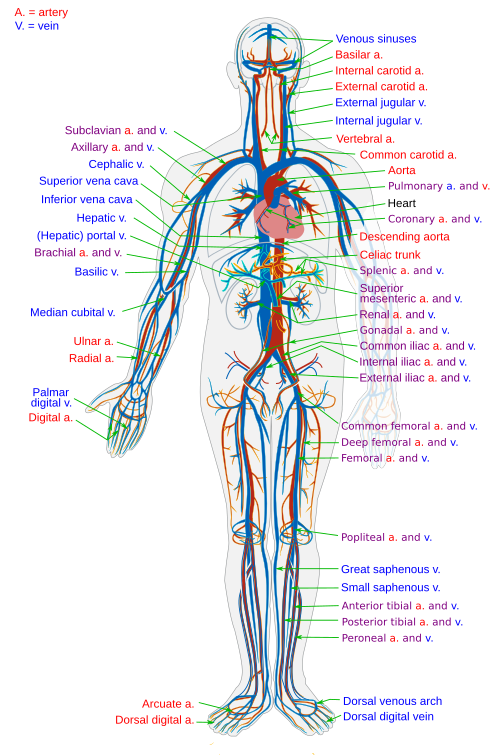
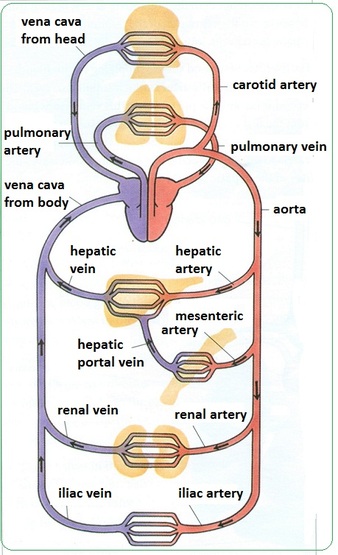
Pulmonary and Systemic Circulation
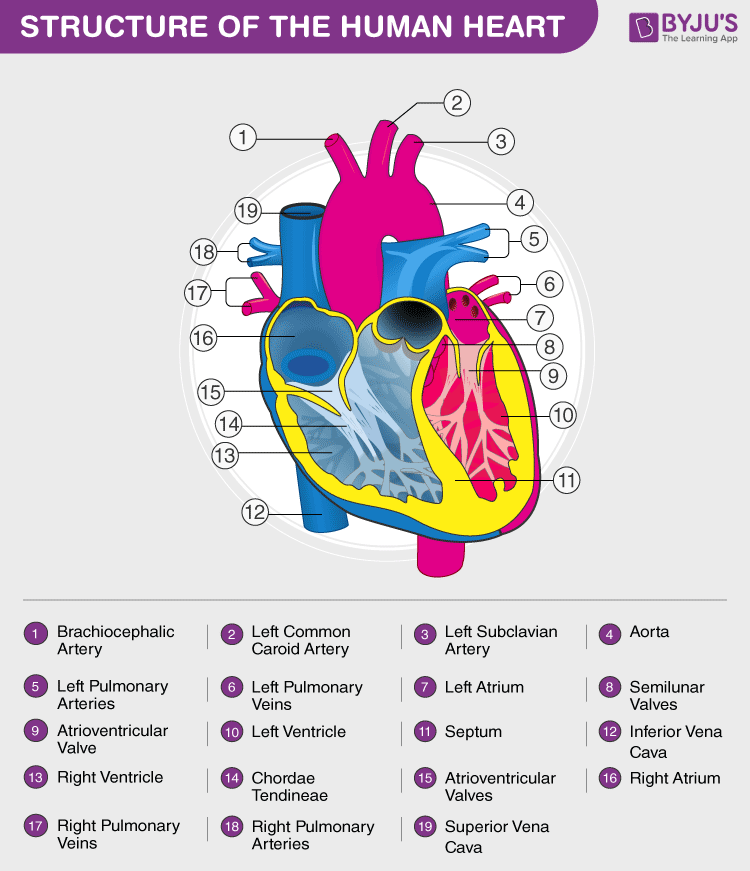
Human Heart Anatomy
Heart Anatomy External
The cardiovascular system is composed of a dual-action muscular pump—the heart—and a closed circuit of blood vessels. Its fundamental biological imperative is the continuous perfusion of tissues, transporting oxygen, nutrients, hormones, and metabolic wastes. To achieve this, the system operates two physically connected but functionally distinct circuits in series.
Figure 1.1: Schematic of the circulation loops.
1.1 The Dual Circulatory System
The heart is functionally divided into right and left halves, each serving a specific vascular network.
Pulmonary vs. Systemic Circulation
The complete circuit ensures that blood alternates between the lungs for gas exchange and the body for nutrient delivery.
The Pulmonary Circuit (Right Side)
This is a relatively short, low-pressure, low-resistance pathway. The right atrium receives oxygen-poor (deoxygenated) blood returning from the systemic tissues via the venae cavae. The right ventricle then pumps this dark red blood into the Pulmonary Trunk, which bifurcates into the pulmonary arteries leading to the lungs. Within the delicate pulmonary capillaries, carbon dioxide is unloaded, and oxygen is bound to hemoglobin. The newly oxygen-rich, bright red blood is returned to the left side of the heart via the pulmonary veins.
The Systemic Circuit (Left Side)
This is a massive, long, high-pressure, high-resistance pathway. The left atrium receives the highly oxygenated blood from the lungs. The left ventricle, possessing the thickest myocardium in the heart, forcefully ejects this blood into the massive Aorta. The aorta distributes this blood through branching systemic arteries to every single organ and capillary bed in the body. After unloading oxygen and collecting wastes, the blood returns to the right side of the heart, completing the cycle.
The Dual Circulatory System and Flow Dynamics
Critical Nomenclature Exception: In systemic circulation, arteries carry oxygenated blood and veins carry deoxygenated blood. However, in the pulmonary circulation, this is completely reversed. The Pulmonary Arteries carry oxygen-poor blood AWAY from the heart to the lungs, while the Pulmonary Veins carry oxygen-rich blood TOWARD the heart.
1.2 Location, Size, and Orientation
The human heart is roughly the size of two hands clasped together (or a large fist). It is safely nestled within the thoracic cavity, specifically within the medial compartment known as the Mediastinum, flanked laterally by the lungs, posterior to the sternum, and anterior to the vertebral column.
Anatomical Landmarks
Orientation: The heart does not sit perfectly straight. It rests obliquely, with approximately two-thirds of its total mass projecting to the left of the midsternal line.
The Base: The broad, flat posterior-superior surface. It is directed toward the right shoulder. All major great vessels (Aorta, Vena Cavae, Pulmonary vessels) emerge from this base.
The Apex: The pointed inferior end, directed anteriorly, inferiorly, and toward the left hip. The apex rests directly upon the superior surface of the diaphragm.
Point of Maximal Intensity (PMI): The exact location where the beating apex of the heart strikes the inner chest wall. Clinically, it is best palpated and auscultated at the 5th intercostal space, just inferior to the left nipple along the midclavicular line.
1.3 The Pericardium (The Protective Sac)
The heart is enclosed in a highly specialized, double-walled sac known as the pericardium. This structure is crucial for protection, anchorage, and frictionless movement.
Layers of the Pericardium and Heart Wall
The anatomic relationship between the tough outer fibrous pericardium, the folding serous pericardium (parietal and visceral layers), the pericardial cavity, and the deeper myocardium.
1. Fibrous Pericardium
The superficial layer composed of extremely tough, dense irregular connective tissue.
Protection: Shields the heart from blunt trauma and prevents the spread of infection from adjacent organs like the lungs.
Anchorage: Physically tethers the heart within the mediastinum (anchored to the diaphragm and sternum).
Prevention of Overfilling: Because this fibrous tissue is highly inelastic, it acts as a physical boundary that strictly limits the expansion of the heart, preventing it from stretching excessively when venous return suddenly increases.
2. Serous Pericardium
A deep, thin, slippery, two-layer membrane forming a closed sac around the heart. It consists of the Parietal Layer (lining the inside of the fibrous pericardium) which folds inward at the base of the heart to become the Visceral Layer (Epicardium), which clings tightly to the external surface of the myocardium.
The Pericardial Cavity & Cardiac Tamponade
The slit-like potential space strictly between the parietal and visceral layers. It contains a thin film of lubricating serous fluid that reduces mechanical friction to almost zero as the heart beats.
Clinical Correlation: Pericarditis is the inflammation of these membranes, creating a harsh "friction rub" sound. If severe inflammation or trauma causes massive amounts of fluid or blood to accumulate rapidly in this cavity, the inelastic fibrous pericardium cannot stretch outward. Instead, the pressure is directed inward, crushing the heart and preventing the ventricles from filling during diastole. This highly lethal condition is known as Cardiac Tamponade.
1.4 Layers of the Heart Wall
Moving inward from the pericardial cavity, the wall of the heart itself is composed of three highly specialized, distinct tissue layers.
Histological Layers of the Heart Wall
A detailed view progressing from the epicardium, through the massively thick myocardium, to the delicate endocardial lining.
1. Epicardium (Visceral Pericardium)
The outermost layer of the heart wall. It is structurally the exact same tissue as the visceral layer of the serous pericardium. It provides a smooth outer surface and is frequently infiltrated with protective adipose (fat) tissue, which cushions the vital coronary blood vessels that traverse the surface of the heart.
2. Myocardium (The Muscle Layer)
The incredibly thick middle layer, composed almost entirely of cardiac muscle cells (cardiomyocytes). This is the layer that physically contracts to generate the pumping force. The cardiac muscle cells are tethered together by a crisscrossing, dense connective tissue network arranged in complex spiral and circular bundles.
The Fibrous Skeleton of the Heart
This dense collagenous network reinforces the myocardium internally and provides rigid, unyielding attachment sites for the cardiac muscle fibers. It serves three paramount functions:
Provides structural support and prevents the heart from tearing itself apart during powerful contractions.
Forms thick, rigid rings around the bases of the four heart valves, preventing the valve openings from stretching and becoming incompetent under extreme pressure.
Electrical Insulation: It physically separates the muscle tissue of the atria from the muscle tissue of the ventricles. Because collagen does not conduct electricity, it prevents action potentials from spreading directly downwards, forcing the electrical signal to travel exclusively through the specialized AV node pathway.
3. Endocardium (The Inner Lining)
The innermost layer of the heart. It is a glistening white sheet of simple squamous epithelium (specifically termed endothelium) resting on a thin connective tissue layer. It lines all the internal heart chambers and covers the fibrous skeleton of the valves. Critically, it is perfectly continuous with the endothelial linings of all the blood vessels entering and leaving the heart, ensuring absolutely smooth, frictionless, non-turbulent blood flow, thereby minimizing the risk of unwanted thrombosis (blood clotting).
Part 2: Chambers, Valves, and the Pathway of Blood
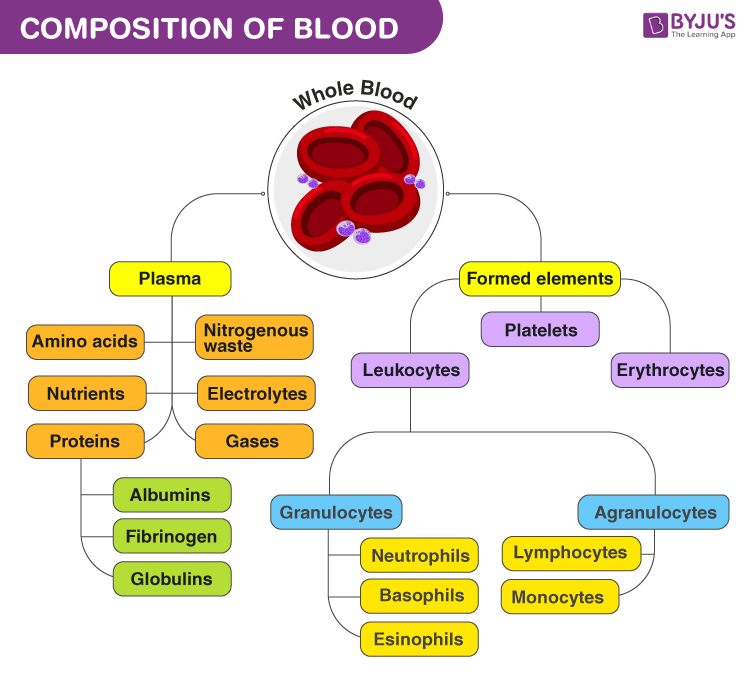
Composition of Blood
Blood Composition Chart
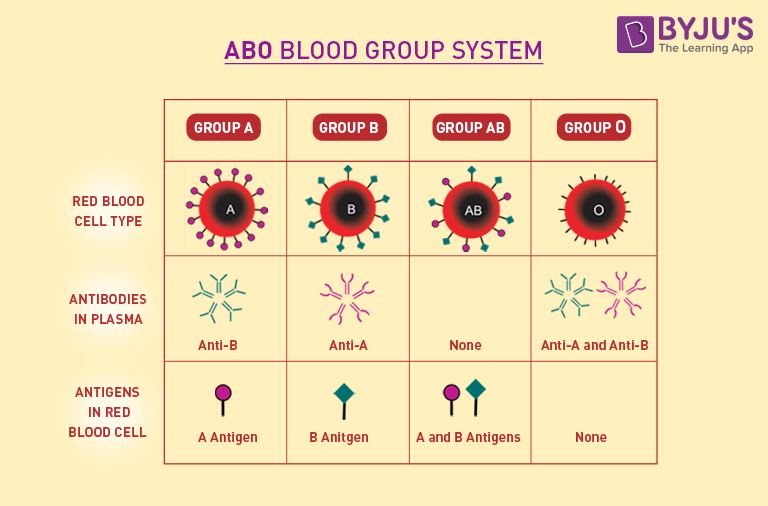
ABO Blood Group System
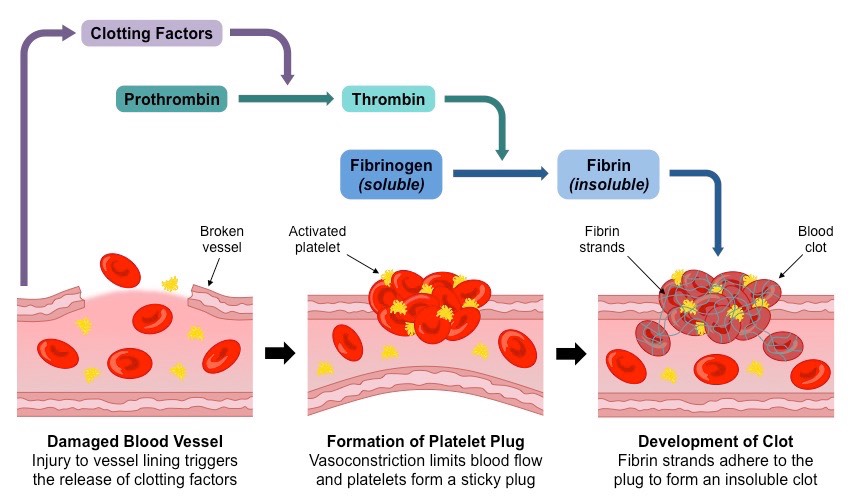
Coagulation Cascade
Coagulation Cascade Details
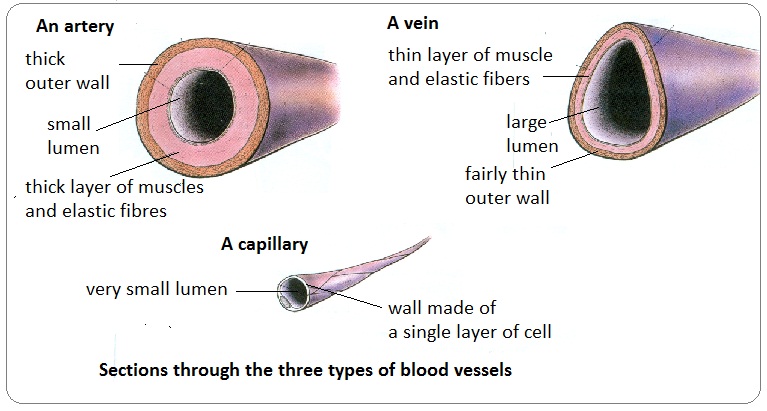
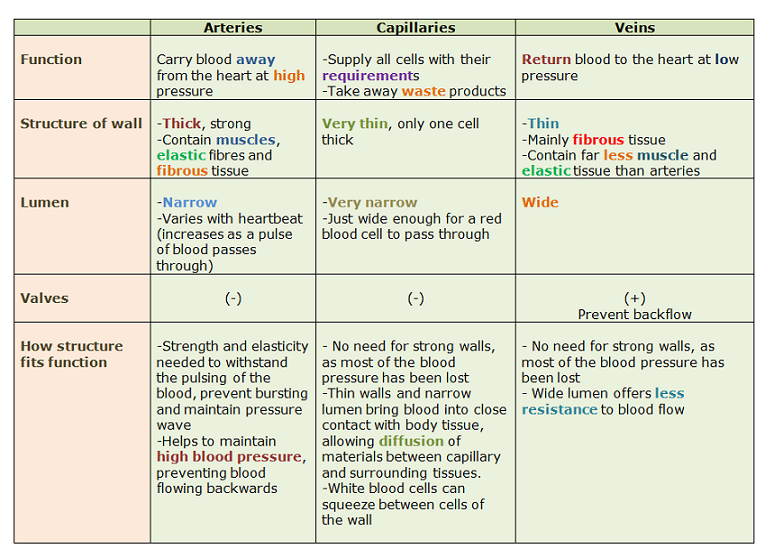
Types of Blood Vessels
Blood Vessel Histology
Artery vs Vein Diagram
Capillary Structure
Capillary Exchange
Heart Anatomy & Circulation
Blood Flow Through the Heart
The heart features four distinct chambers: two superior receiving chambers (the Atria) and two inferior discharging chambers (the Ventricles). An intricate, highly durable system of four one-way valves strictly enforces the unidirectional flow of blood through these chambers, preventing fatal backflow.
2.1 The Atria: The Receiving Chambers
The atria are relatively small, thin-walled chambers because their primary duty is simply to receive blood returning to the heart and pass it down into the ventricles immediately below them. Gravity does most of the work; the atria only need to contract minimally to push the final 20% of blood into the ventricles (the "atrial kick"). Both atria possess small, wrinkled, protruding appendages called Auricles, which slightly increase their internal volume capacity.
Right Atrium
Receives oxygen-poor (deoxygenated) blood returning from the entire systemic circulation. It features three major venous openings:
Superior Vena Cava (SVC): Returns blood from body regions superior to the diaphragm.
Inferior Vena Cava (IVC): Returns blood from body areas inferior to the diaphragm.
Coronary Sinus: Returns venous blood collected from the myocardium of the heart itself.
The inner anterior wall features parallel muscle ridges called Pectinate Muscles. The interatrial septum bears a shallow depression called the Fossa Ovalis, a remnant of the fetal foramen ovale.
Left Atrium
Receives highly oxygenated, bright red blood returning directly from the lungs. Its internal surface is mostly smooth.
Receives blood via four Pulmonary Veins (two right and two left).
Pumps blood downward through the Mitral valve directly into the massive left ventricle.
2.2 The Ventricles: The Discharging Pumps
The ventricles are the massive, thick-walled, actual muscular pumps of the heart. Their forceful contractions propel blood out of the heart and into the immense arterial networks. The internal walls of both ventricles feature irregular muscle ridges called Trabeculae Carneae and cone-like Papillary Muscles which project into the cavity to anchor valve strings.
Notice the dramatic difference in myocardial thickness between the right and left ventricles, a perfect example of anatomy dictating physiology.
Right vs. Left Ventricular Workload
It is a critical physiological fact that both the Right and Left Ventricles pump exactly the same volume of blood with every single beat (the Stroke Volume, typically ~70 mL). However, their physical workloads are vastly different.
The Right Ventricle pumps blood into the Pulmonary Trunk, destined for the lungs. This is a short, low-pressure, low-resistance circuit. Therefore, its wall is relatively thin, and it is crescent-shaped, wrapping around the left ventricle.
The Left Ventricle pumps blood into the Aorta, destined for the entire body. This is an enormously long, high-pressure, extremely high-resistance circuit. To overcome this massive systemic vascular resistance (Afterload), the left ventricle must generate immense pressure. Consequently, its myocardium is roughly three times thicker than that of the right ventricle, and it is perfectly circular to maximize pumping force.
2.3 The Four Heart Valves & Their Mechanics
Blood is a fluid, and it flows entirely driven by pressure gradients—from areas of high pressure to areas of low pressure. The four heart valves are entirely passive mechanical devices; they contain no muscle tissue themselves and cannot "actively" open or close. They are forced open and slammed shut strictly by differences in blood pressure on their two sides.
1. Atrioventricular (AV) Valves
Located at the junctions between the atria and their respective ventricles. Their sole purpose is to prevent the backflow of blood upward into the atria when the ventricles forcefully contract.
Tricuspid Valve: Features 3 flexible cusps. Located between the Right Atrium and Right Ventricle.
Bicuspid (Mitral) Valve: Features 2 cusps. Located between the Left Atrium and Left Ventricle. It resembles a bishop's miter (tall hat).
Support Structure of the AV Valves
The crucial anatomic relationship between the valve cusps, chordae tendineae, and papillary muscles.
Mechanical Operation (The Guy-Wire System):
Attached to the free edges of the AV valve cusps are tiny, immensely strong white collagen cords called Chordae Tendineae ("heart strings"). These cords anchor the cusps downward to the Papillary Muscles protruding from the ventricular walls.
When the ventricles are relaxed (diastole), blood falls from the atria, pushing the AV valves open passively. The chordae tendineae hang slack. However, when the ventricles contract (systole), ventricular pressure skyrockets, violently forcing blood upward against the AV valve flaps, slamming them shut. Simultaneously, the papillary muscles contract, pulling the chordae tendineae completely taut. This prevents the immense pressure from blowing the valve flaps inside-out (everting) back into the atria, much like holding onto the strings of an umbrella in a hurricane.
2. Semilunar (SL) Valves
Located at the bases of the large arteries exiting the ventricles. They prevent arterial blood from washing back down into the ventricles after contraction ends.
Pulmonary Semilunar Valve: Guards the base of the Pulmonary Trunk (exiting the Right Ventricle).
Aortic Semilunar Valve: Guards the base of the immense Aorta (exiting the Left Ventricle).
Valve Actions During Systole and Diastole
Note how the AV and Semilunar valves act reciprocally. When AV valves are open, Semilunar valves are closed, and vice versa.
Mechanical Operation (The Pocket System):
Each SL valve is fashioned from three pocket-like, half-moon shaped cusps. They do not possess chordae tendineae. When the ventricles contract, the immense pressure forces blood upward, physically flattening the SL cusps outward against the arterial walls, opening the pathway wide. When the ventricles relax, the pressure inside them drops precipitously. The high-pressure blood in the aorta and pulmonary trunk immediately begins to flow backward toward the low-pressure heart. This backflowing blood instantly fills the three cup-like pockets of the SL valves, ballooning them out until their edges meet tightly in the center, snapping the valves securely shut and preventing any regurgitation into the ventricles.
Part 3: Coronary Circulation & Ischemic Heart Disease
The heart muscle (myocardium) is far too thick for oxygen and nutrients to simply diffuse from the blood pooling inside the chambers to reach the deeper cardiac cells. Therefore, the heart requires its own dedicated, private blood supply: the Coronary Circulation. It is the shortest functional circulation in the human body. Paradoxically, the coronary vessels deliver blood to the myocardium primarily when the heart is relaxed (diastole), because during active contraction (systole), the contracting muscle physically compresses the coronary vessels, severely restricting blood flow.
3.1 Anatomy of the Coronary Arteries and Veins
The Left and Right Coronary Arteries arise directly from the base of the aorta, just superior to the cusps of the aortic semilunar valve. They encircle the heart in the coronary sulcus (atrioventricular groove), sending major branches down the external ventricular walls.
Left Coronary Artery (LCA)
Runs toward the left side of the heart and immediately divides into two major branches:
Anterior Interventricular Artery: Clinically universally known as the LAD (Left Anterior Descending). It courses down the anterior interventricular sulcus, supplying the anterior walls of both ventricles and the critical interventricular septum (which houses the bundle branches). It is notoriously called the "widowmaker" because sudden occlusion here usually causes a massive, fatal heart attack.
Circumflex Artery (LCx): Follows the coronary sulcus around to the posterior side, supplying the left atrium and the posterior wall of the left ventricle.
Right Coronary Artery (RCA)
Courses to the right side of the heart in the coronary sulcus, supplying the right atrium and nearly all the right ventricle via two primary branches:
Right Marginal Artery: Supplies the lateral right side of the myocardium.
Posterior Interventricular Artery (PDA): Runs to the heart apex on the posterior side, supplying the posterior ventricular walls. Near the apex, it eventually merges (anastomoses) with the distal ends of the LAD.
Clinical Note: The RCA also crucially supplies blood to the SA node and AV node in the vast majority of people. RCA occlusion can thus cause severe bradycardia or heart blocks.
Coronary Venous Drainage: The Coronary Sinus
After passing through the massive myocardial capillary beds, deoxygenated venous blood is collected by the Great, Middle, and Small Cardiac veins. These veins converge on the posterior aspect of the heart to form a massive, enlarged vessel called the Coronary Sinus, which empties this deoxygenated blood directly into the Right Atrium.
3.2 Ischemic Heart Disease & Atherosclerosis
Coronary Artery Disease (CAD) is caused by a progressive narrowing of the coronary vessels, critically reducing the blood and oxygen supply to the hard-working heart muscle, a state known as Ischemia.
The Progression of Atherosclerosis
Atherosclerosis begins with endothelial injury, followed by the massive accumulation of LDL cholesterol and macrophages in the intimal wall. These form a lipid-rich "fatty streak" which hardens into a fibrous atherosclerotic plaque. This plaque physically encroaches upon the lumen, obstructing blood flow. If the unstable plaque ruptures, it instantly triggers the clotting cascade, forming a thrombus that completely occludes the artery.
Angina Pectoris vs. Myocardial Infarction
Angina Pectoris
Literal translation: "choked chest". It is severe thoracic pain caused by a fleeting, temporary deficiency in blood delivery to the myocardium.
The myocardial cells are weakened by acute hypoxia and switch to anaerobic glycolysis (producing lactic acid, which stimulates pain receptors), but critically, the cells do not die. The pain is often triggered by physical exertion or emotional stress (which increase myocardial oxygen demand) and is relieved by rest or sublingual nitroglycerin (a potent vasodilator).
Myocardial Infarction (MI)
Commonly called a "Heart Attack". Occurs when a coronary blockage (often from a ruptured plaque triggering a thrombus) is profound, complete, and prolonged.
The severe lack of oxygen results in the irreversible death (necrosis) of the ischemic myocardial cells. Because adult cardiac muscle cells are almost entirely amitotic (they cannot undergo cell division to regenerate), the dead contractile tissue is eventually cleared by macrophages and permanently replaced by non-contractile, rigid fibrous scar tissue. The severity of the MI depends heavily on the size and location of the infarct.
3.3 Therapeutic Interventions for Coronary Occlusion
Modern cardiology offers several mechanical and surgical interventions to physically restore perfusion (revascularization) to the ischemic heart tissue before it undergoes necrosis.
Coronary Artery Bypass Graft (CABG)
An invasive open-heart surgical procedure. A healthy blood vessel (frequently the great saphenous vein harvested from the leg, or the internal mammary artery) is surgically grafted onto the heart. One end is attached to the aorta, and the other end is attached past the blockage, literally creating a detour or "bypass" around the obstructed section to supply the starving tissue below.
Angioplasty & Stent Placement (PCI)
Percutaneous Coronary Intervention. A minimally invasive procedure where a catheter equipped with a tiny balloon is threaded through the peripheral arterial system (via the femoral or radial artery) directly into the obstructed coronary artery. The balloon is inflated at extremely high pressure, physically squashing the atherosclerotic plaque flat against the vessel wall to widen the lumen. A tiny wire mesh tube (a Stent) is deployed to permanently hold the artery open.
Part 4: Cardiac Muscle Histology & The Conduction System
Cardiac Conduction System
Cardiac Action Potential
4.1 Microscopic Anatomy of Cardiac Muscle
Cardiac muscle tissue is utterly unique. Like skeletal muscle, it is striated (due to the highly organized arrangement of actin and myosin sarcomeres). However, cardiac cells are short, fat, branched, and interconnected. Crucially, they possess massive, numerous mitochondria (accounting for ~25-35% of total cell volume), making them highly resistant to fatigue and utterly dependent on continual aerobic respiration.
Intercalated Discs (IMAT High-Yield)
Cardiac cells interlock tightly at specialized, dark-staining junctions called Intercalated Discs. These complex junctions contain two critically important structural elements that ensure the heart acts as a single, unified organ.
1. Desmosomes
Mechanical anchoring junctions. They act like heavy-duty molecular rivets, firmly holding the adjacent cells together so they are not torn apart under the immense physical stress of continuous, forceful contraction.
2. Gap Junctions
Microscopic communicating pores that allow ions to pass freely from the cytoplasm of one cell directly into the next. This electrically couples the entire myocardium. Because action potentials travel seamlessly through gap junctions, the entire myocardium acts as a single coordinated unit—a Functional Syncytium. (If one cell is stimulated, they all contract together).
4.2 The Intrinsic Conduction System
Unlike skeletal muscle, the heart does not depend on the nervous system to initiate its beat. It possesses intrinsic Autorhythmicity. Approximately 1% of cardiac fibers are specialized, non-contractile autorhythmic (pacemaker) cells. They possess unstable resting membrane potentials (pacemaker potentials) that continuously and automatically drift toward threshold, initiating action potentials that spread throughout the heart to coordinate the contraction sequence.
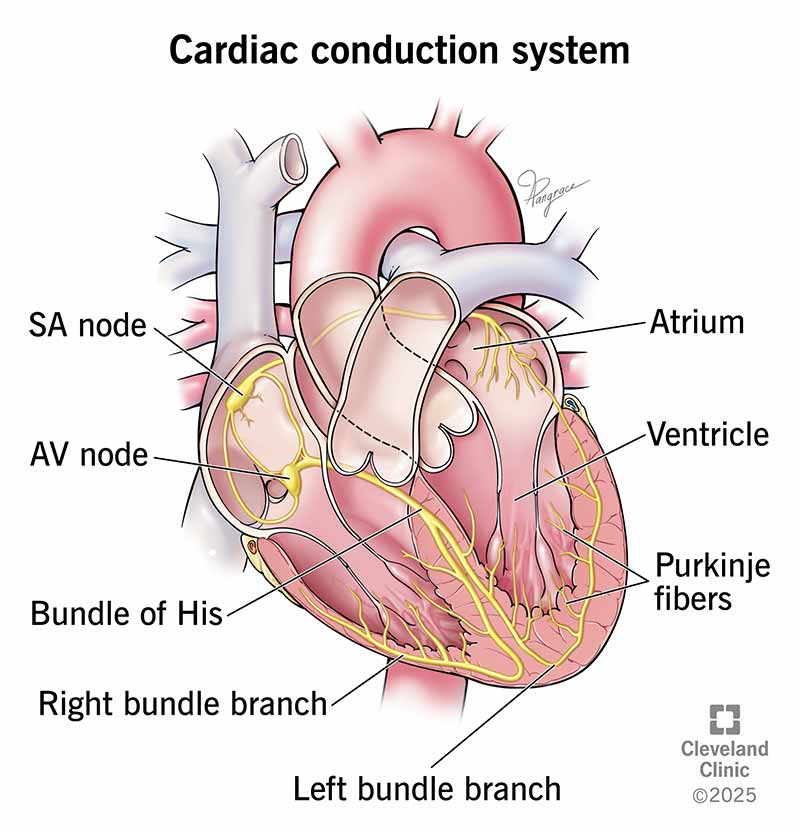
The Cardiac Conduction System Anatomy
The electrical sequence forces the atria to contract first, pushing blood downwards, followed by the ventricles contracting from the apex upwards, pushing blood out into the great arteries.
The Pacemaker Pathway (Sequence of Excitation)
Sinoatrial (SA) Node: Located in the superior wall of the right atrium. It is the primary Pacemaker of the normal heart. It sets the pace because its cells automatically depolarize faster than any other part of the system (inherent rate of ~100 bpm, tempered to ~75 bpm by vagal tone). It generates the impulse that spreads across both atria via gap junctions, causing them to contract in unison.
Atrioventricular (AV) Node: Located at the inferior interatrial septum. Here, the electrical impulse is intentionally delayed by about 0.1 seconds. Crucial Physiological Function: This critical delay allows the atria to completely finish contracting and empty their final load of blood into the ventricles BEFORE the ventricles are stimulated to begin their powerful contraction. Without this delay, blood would be pumped against closed valves.
Atrioventricular (AV) Bundle (Bundle of His): Located in the superior part of the interventricular septum. It is the ONLY electrical connection between the atria and the ventricles. The fibrous skeleton insulates the rest of the AV junction, preventing stray electrical signals from causing chaotic simultaneous contractions.
Right and Left Bundle Branches: The AV bundle splits into these two pathways, which course straight down either side of the interventricular septum toward the apex of the heart.
Purkinje Fibers (Subendocardial Conducting Network): These large barrel-shaped fibers penetrate deep into the heart apex and then turn superiorly, branching extensively into the massive ventricular walls. They rapidly distribute the impulse to the bulk of the ventricular myocardium. Because the signal starts at the apex and moves up, the ventricles contract in a wringing motion from the bottom up, efficiently forcing blood superiorly out into the great arteries.
4.3 The Cardiac Action Potential & The Plateau Phase
The action potential of contractile cardiac muscle cells is fundamentally different from that of skeletal muscle or neurons due to the presence of a prolonged Plateau Phase.
Cardiac Action Potential and the Plateau
Phases of the Action Potential:Phase 0 (Depolarization): Fast voltage-gated $Na^+$ channels open. Rapid influx of Sodium. Phase 2 (Plateau Phase):Slow, L-type Calcium ($Ca^{2+}$) channels open, allowing a steady influx of $Ca^{2+}$ from the extracellular fluid. This positive influx balances the efflux of Potassium ($K^+$), keeping the membrane potential depolarized (near 0 mV) for a prolonged period (approx. 200 ms). Phase 3 (Repolarization): Calcium channels close, and voltage-gated Potassium channels fully open, rapidly returning the cell to its resting negative potential.
Physiological Significance of the Plateau (IMAT Concept)
The plateau phase drastically extends the Absolute Refractory Period (the time during which a cell cannot be re-stimulated) of cardiac muscle to almost match the duration of the mechanical contraction itself. This prevents the heart from undergoing tetanus (sustained, continuous tetanic contraction). If the heart muscle were to undergo tetanus, it would lock up and be unable to relax. The heart MUST relax (diastole) in order to fill with blood for the next beat. The plateau guarantees this relaxation phase.
Part 6: Electrocardiography (ECG) & The Cardiac Cycle
Basic ECG waveform
Cardiac Cycle Diagram
6.1 The Electrocardiogram (ECG / EKG)
The electrical currents generated by the autorhythmic nodes and transmitted through the contracting myocardium spread throughout the body fluids and can be detected by electrodes placed on the skin. An ECG is a composite graphic record of ALL the electrical action potentials generated by nodal and contractile cells at a given time. It is vital to remember: An ECG records ONLY electrical events, NOT the physical mechanical muscle contractions (though the electrical events immediately precede the mechanical ones).
A Normal ECG Tracing and Intervals
The ECG is divided into distinct waves and intervals that correspond precisely to the spread of the electrical signal through the heart.
P Wave
Represents: Atrial Depolarization
A small upward deflection resulting from the SA node firing. The depolarization wave spreads across the atria. Approximately 0.1 seconds after the P wave begins, the atria physically contract (atrial systole).
QRS Complex
Represents: Ventricular Depolarization
A large, sharp, rapidly changing spike. The electrical signal sweeps down the bundle branches and out through the Purkinje fibers. It precedes massive ventricular contraction.
Note: Atrial repolarization also happens at this exact moment, but its weak electrical signal is completely masked by the massive QRS voltage.
T Wave
Represents: Ventricular Repolarization
A broad, dome-shaped wave occurring as the ventricles electrically reset, happening just before ventricular relaxation (diastole). It is wider than the QRS because repolarization is a slower process than depolarization.
Critical Clinical Intervals:
P-R Interval: The time from the beginning of atrial excitation to the beginning of ventricular excitation. It includes the vital 0.1-second delay at the AV node. An abnormally long P-R interval often indicates a heart block (damage to the AV node).
S-T Segment: The entire ventricular myocardium is depolarized (in the plateau phase). In patients experiencing acute myocardial ischemia or infarction, this segment is famously elevated (STEMI) or depressed.
6.2 The Cardiac Cycle (Mechanics of Pumping)
The cardiac cycle includes all the mechanical events associated with the blood flow through the heart during one complete heartbeat. Blood flow through the heart is driven entirely by pressure changes within the chambers. Blood always flows down its pressure gradient, and valves act as doors to ensure it flows only one way.
Terminology Key: Systole means contraction (high pressure). Diastole means relaxation (low pressure/filling).
Phases of the Cardiac Cycle (Starting at Mid-Diastole)
1. Ventricular Filling (Mid-to-Late Diastole):
Pressure in the heart is very low. Blood returning from circulation flows passively through the atria and open AV valves directly into the ventricles. The Aortic and Pulmonary semilunar valves are closed. Roughly 80% of ventricular filling occurs passively. At the end of this phase, the SA node fires (P wave), the atria contract (atrial systole), squeezing the remaining 20% of blood into the ventricles (the "atrial kick"). The ventricles now contain their absolute maximum volume for the cycle, called the End Diastolic Volume (EDV) (typically ~120 ml).
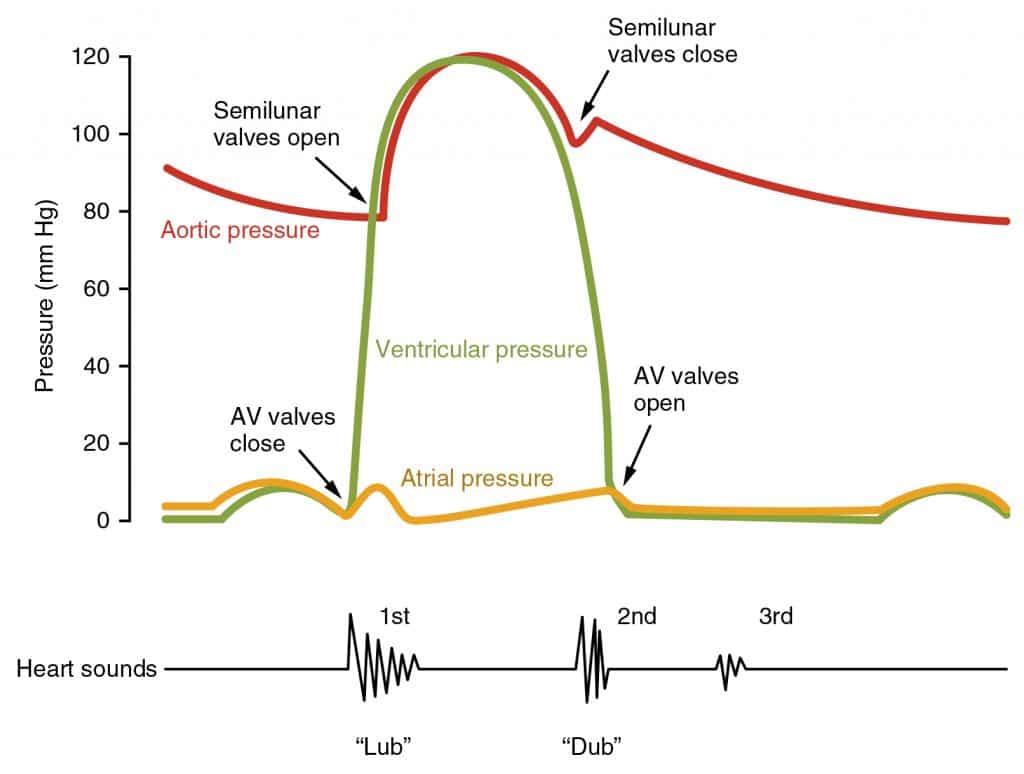
2. Ventricular Systole (Atria in Diastole):
Ventricles begin to electrically depolarize (QRS complex) and then mechanically contract. Pressure inside the ventricles rises sharply, instantly exceeding atrial pressure and slamming the AV valves shut (creating the 1st Heart Sound).
A. Isovolumetric Contraction Phase:
For a split second, the AV valves are closed, but the ventricular pressure is not yet high enough to blow the Semilunar valves open against the immense arterial back-pressure. The ventricle is a completely closed chamber. Volume stays exactly the same (isovolumetric) while pressure skyrockets dramatically.
B. Ventricular Ejection Phase:
Ventricular pressure finally exceeds the pressure in the large arteries (aorta > 80 mmHg). The Semilunar valves are violently blown open. Blood rushes out of the ventricles into the aorta and pulmonary trunk.
3. Isovolumetric Relaxation (Early Diastole):
Ventricles repolarize (T wave) and relax. Ventricular pressure drops rapidly. Blood remaining in the aorta and pulmonary trunk flows backwards momentarily towards the low-pressure ventricles, catching the cusps and snapping the Semilunar valves shut (creating the 2nd Heart Sound). The volume of blood left behind in the ventricle after it has finished contracting is called the End Systolic Volume (ESV) (typically ~50 ml). The AV valves are still closed until ventricular pressure drops below atrial pressure, at which point they open, restarting the cycle.
Left Ventricular Pressure-Volume Loop (PV Loop)
The PV loop mathematically charts a single cardiac cycle. The bottom right corner represents EDV (maximum volume before contraction). The top left corner represents ESV (minimum volume after contraction). The horizontal width of the entire loop represents the Stroke Volume (SV). The vertical height represents the immense pressure generated during systole.
Listening with a stethoscope reveals two distinct sounds per heartbeat. It is paramount to understand that these sounds are NOT the cardiac muscles contracting; they are the acoustic vibrations caused by the turbulence of blood when the valves snap shut.
Heart Valve Auscultation Sites
Physicians do not listen directly over the valves. They place the stethoscope downstream from the valves, where the sound of the turbulent blood flow echoes best onto the chest wall. (e.g., Aortic valve is heard at the 2nd intercostal space at the right sternal margin).
1st Sound ("Lubb")
Occurs when the AV valves (Tricuspid & Mitral) close at the very beginning of ventricular systole. It tends to be louder, longer, and more resonant.
2nd Sound ("Dup")
Occurs when the Semilunar valves (Aortic & Pulmonary) close at the beginning of ventricular diastole. It is a shorter, sharper sound.
Clinical Note: Heart Murmurs
Abnormal or unusual heart sounds. They usually indicate severe valve problems. An incompetent (leaky) valve allows backflow, creating a swishing sound. A stenotic (narrowed, stiff) valve forces blood through a tiny opening, creating a high-pitched click or screech.
Part 7: Cardiac Output & Advanced Hemodynamics
Hemodynamics and Blood Pressure
To truly understand cardiovascular physiology, one must master the mathematical relationships and variables that define the heart's pumping efficiency. The heart is highly responsive, continuously adjusting its output to match the body's metabolic demands for oxygen and nutrient delivery.
7.1 Defining Cardiac Output (CO)
Cardiac Output (CO) is defined as the total volume of blood pumped by each ventricle in one minute. It is the fundamental measure of overall cardiac performance. CO is calculated as the product of Heart Rate (HR) and Stroke Volume (SV).
$$ CO = HR \times SV $$
Normal resting CO is approximately 5.25 Liters/min (75 beats/min $\times$ 70 ml/beat).
This means the entire blood volume of a human body passes through each side of the heart every single minute!
During strenuous exercise, the heart massively increases both HR and SV, causing CO to surge to 25-35 L/min to supply working muscles.
Stroke Volume (SV) is the precise volume of blood pumped out by one ventricle with each single beat. It correlates strongly with the force of ventricular contraction. Mathematically, it is simply the difference between the volume you start with and the volume left behind:
$$ SV = EDV - ESV $$
End Diastolic Volume (EDV): The volume of blood in the ventricle just before it contracts (when it is maximally full after diastole). Usually ~120 ml.
End Systolic Volume (ESV): The volume of blood remaining in the ventricle after it has finished its forceful contraction. Usually ~50 ml.
Therefore, SV = 120ml - 50ml = 70 ml per beat.
7.2 Three Crucial Factors Affecting Stroke Volume
To alter Cardiac Output to meet varying metabolic demands, the body manipulates Stroke Volume by continuously adjusting three incredibly important physiological variables: Preload, Contractility, and Afterload.
1. Preload (Stretch)
Preload is the degree of stretch of cardiac muscle cells just before they contract. It is directly proportional to EDV (how much blood fills the heart).
Frank-Starling Law of the Heart:
"The more the heart fills with blood during diastole, the greater the force of contraction during systole."
Mechanism: Stretching the muscle fibers (by increasing Venous Return) optimally aligns the actin and myosin filaments within the sarcomeres. This optimal overlap allows a maximum number of cross-bridges to form, resulting in a significantly more powerful contraction and a higher Stroke Volume. It acts like a rubber band: the more you pull it, the harder it snaps back.
The contractile strength achieved at a given muscle length. It is independent of muscle stretch or EDV. It controls how much blood is left behind (ESV).
Vigorously increased by sympathetic nervous system stimulation (Epinephrine/Norepinephrine), which act as positive inotropes.
These hormones bind to Beta-1 receptors, activating a cAMP second-messenger system that opens massive numbers of calcium channels in the cell membrane.
The massive influx of $Ca^{2+}$ exposes drastically more actin binding sites, resulting in an explosive, highly forceful contraction.
A stronger contraction pushes a larger percentage of blood out of the heart, leaving far less blood behind in the chamber.
The immense 'back pressure' that the ventricles must overcome in order to force the semilunar valves open and eject blood into the aorta and pulmonary trunk.
It is essentially equivalent to the systemic arterial blood pressure.
In healthy individuals, it is relatively constant and not a major determinant of altering SV.
Clinical Pathology: In patients suffering from Hypertension (High BP), the afterload is disastrously huge. The ventricles must exert immense effort and consume vast amounts of oxygen just to pry open the aortic valve, leaving far less energy and time to actually eject the blood.
While the SA node strictly dictates the intrinsic baseline rhythm of the heart, the Autonomic Nervous System continuously modulates this rate, functioning precisely like the accelerator and brakes of a car depending on the body's moment-to-moment needs.
Sympathetic Nervous System (The Accelerator)
The Cardioacceleratory center in the Medulla sends signals down the spinal cord to the sympathetic trunk ganglia. Postganglionic fibers release Norepinephrine directly at the SA node, AV node, and heavily into the ventricular myocardium.
This catecholamine binds to Beta-1 receptors, causing $Na^+$ and $Ca^{2+}$ channels to open. This lowers the threshold for firing, causing the pacemaker cells to depolarize much more rapidly.
Result: Increases Heart Rate (Tachycardia) AND Increases Contractility.
Parasympathetic Nervous System (The Brakes)
The Cardioinhibitory center in the Medulla sends signals primarily via the massive Vagus Nerves (Cranial Nerve X). They release Acetylcholine (ACh) at the SA and AV nodes.
ACh binds to Muscarinic receptors, which opens $K^+$ channels, causing potassium to rush out of the cell. This hyperpolarizes the pacemaker cells. They take much longer to drift back up to threshold.
Result: Decreases Heart Rate (Bradycardia). At rest, constant Vagal tone keeps the heart rate at a calm ~75 bpm instead of the SA node's intrinsic racing pace of 100 bpm.
Part 8: Blood Vessels & Blood Pressure Regulation
Blood is pumped by the heart, but it is the dynamic, living network of blood vessels that directs this flow, maintains the necessary pressure, and facilitates the ultimate goal of the entire system: capillary exchange.
8.1 Vessel Histology & Classification
All blood vessels (except the microscopic capillaries) are composed of three distinct histological layers (tunics) surrounding a central blood-containing space, the lumen.
Histological Structure: Artery vs. Vein vs. Capillary
Notice the extreme thickness of the Tunica Media in the artery to withstand high pressure, compared to the large lumen and thin walls of the vein. Capillaries consist solely of the Tunica Intima to allow for rapid diffusion.
The Three Tunics (Layers)
1. Tunica Intima (Innermost)
Contains the endothelium (simple squamous epithelium) that lines the lumen of all vessels. It forms a slick surface that minimizes friction as blood moves through.
2. Tunica Media (Middle)
The thickest layer in arteries. Consists of circularly arranged smooth muscle cells and sheets of elastin. Regulated by the sympathetic nervous system, this layer bears the chief responsibility for maintaining blood pressure and continuous blood circulation by undergoing vasoconstriction (lumen reduction) or vasodilation (lumen widening).
3. Tunica Externa / Adventitia (Outermost)
Composed largely of loosely woven collagen fibers that protect and reinforce the vessel, anchoring it to surrounding structures. In large vessels, it contains its own system of tiny blood vessels called the vasa vasorum.
8.2 Types of Capillaries
Capillaries are the exchange vessels. They form intricate networks (capillary beds) between arterioles and venules. Based on their permeability, they are classified into three types.
The Three Types of Capillaries
Continuous Capillaries: The most common and least permeable. Endothelial cells provide an uninterrupted lining, connected by tight junctions. Abundant in skin and muscles. In the brain, these tight junctions are highly complete, forming the structural basis of the Blood-Brain Barrier.
Fenestrated Capillaries: The endothelial cells contain numerous oval pores (fenestrations). Much more permeable to fluids and small solutes. Found wherever active capillary absorption or filtrate formation occurs (e.g., small intestines, endocrine glands, and the filtration membranes of the kidneys).
Sinusoidal Capillaries: The most highly permeable, leaky capillaries. They have large, irregularly shaped lumens, huge fenestrations, and massive intercellular clefts. They allow extremely large molecules and even entire blood cells to pass between the blood and surrounding tissues. Found only in the liver, bone marrow, spleen, and adrenal medulla.
8.3 Venous Return Mechanisms
Blood pressure in the venous system is incredibly low—often near 0 mmHg by the time it reaches the venae cavae. This low pressure is insufficient to overcome gravity and return blood from the legs to the heart. Therefore, veins possess special adaptations to assist venous return.
Venous Valves
Veins contain delicate, flap-like valves (formed from folds of the tunica intima) that resemble the semilunar valves of the heart. They allow blood to flow upward toward the heart but snap shut if gravity attempts to pull the blood backward. If these valves become incompetent and fail, blood pools, resulting in enlarged, tortuous Varicose Veins.
The Skeletal Muscle Pump
As skeletal muscles (especially in the legs) contract and relax during movement, they physically squeeze the deep veins running between them. This "milks" the blood upward past the valves toward the heart. Standing perfectly still for long periods removes this pump, causing blood to pool in the legs and potentially leading to fainting.
8.4 Blood Pressure Regulation
Maintaining adequate blood pressure (Mean Arterial Pressure, or MAP) is vital to ensure tissue perfusion. $$ MAP = CO \times TPR $$ (where TPR is Total Peripheral Resistance). Blood pressure is strictly controlled by a combination of short-term neural controls and long-term hormonal controls.
1. Short-Term Neural Control: The Baroreceptor Reflex
Neural controls operate via reflex arcs involving baroreceptors, the cardiovascular center of the medulla, and autonomic fibers to the heart and vascular smooth muscle. They alter blood pressure instantly (within seconds) by changing TPR and CO, usually in response to postural changes (like standing up quickly).
Mechanism of Action:
Baroreceptors are stretch-sensitive mechanoreceptors located strategically in the Carotid Sinuses (protecting blood supply to the brain) and the Aortic Arch (protecting systemic supply).
When BP rises: The vessels stretch, stimulating the baroreceptors. They send rapid impulses to the vasomotor center in the medulla, inhibiting it (causing vasodilation and a drop in TPR). They also stimulate the cardioinhibitory center (increasing vagal parasympathetic tone to the SA node), which drops the heart rate and CO. Blood pressure falls back to normal.
When BP drops: Baroreceptors are stretched less, sending fewer impulses. The vasomotor center is released from inhibition, causing rapid sympathetic vasoconstriction (raising TPR). The cardioacceleratory center fires, raising HR and contractility. Blood pressure rises back to normal.
2. Long-Term Hormonal Control: The RAAS Pathway
While neural reflexes act quickly to change vessel diameter, they eventually adapt to chronic high or low pressure. Long-term regulation is handled entirely by the kidneys, which alter blood volume. The most potent mechanism is the Renin-Angiotensin-Aldosterone System (RAAS).
The Complete RAAS Cascade (IMAT Critical Pathway):
When systemic blood pressure drops precipitously (e.g., from severe hemorrhage or dehydration), specialized cells in the kidneys detect this drop and release the enzyme Renin into the blood.
Renin acts upon Angiotensinogen (a plasma protein continuously produced by the liver), cleaving it to form Angiotensin I.
As Angiotensin I flows through the extensive capillary beds of the lungs, an enzyme called ACE (Angiotensin-Converting Enzyme) converts it into the active hormone Angiotensin II.
Angiotensin II is one of the most potent vasoconstrictors in the human body. It instantly constricts systemic arterioles, causing a massive spike in TPR and blood pressure.
Furthermore, Angiotensin II stimulates the adrenal cortex to secrete the steroid hormone Aldosterone.
Aldosterone targets the kidney tubules, forcing them to intensely reabsorb Sodium ($Na^+$). Water obligatorily follows the sodium via osmosis back into the bloodstream. This dramatically increases the physical volume of blood, raising blood pressure long-term.
8.5 Capillary Exchange & The Lymphatic System
The entire purpose of the cardiovascular system is fulfilled at the capillary beds: the exchange of gases, nutrients, and fluids between the blood and the interstitial fluid surrounding the cells. This fluid movement is driven by opposing physical forces known as Starling Forces.
1. Capillary Hydrostatic Pressure (CHP)
This is essentially the capillary blood pressure. It is the physical force exerted by the fluid against the capillary wall. It is the primary force that PUSHES fluid out of the capillary and into the tissue spaces (Filtration). It is highest at the arterial end of the capillary bed and drops lower at the venous end.
2. Blood Colloid Osmotic Pressure (BCOP)
This is the osmotic force created by the presence of large, non-diffusible plasma proteins (primarily Albumin) trapped inside the capillary. Because there are more proteins inside the blood than outside in the tissue fluid, water tries to move via osmosis back into the blood. This force PULLS fluid back into the capillary (Reabsorption). This force remains constant across the entire capillary bed.
At the arterial end, Hydrostatic pressure > Osmotic pressure, so fluid is forced OUT. At the venous end, Hydrostatic pressure drops, so Osmotic pressure dominates, pulling fluid IN. However, slightly more fluid is pushed out than is pulled back in. If left alone, tissues would swell catastrophically with edema.
Interaction of the Lymphatic and Cardiovascular Systems
The Lymphatic System acts as a vital drainage network. Extremely permeable blind-ended lymphatic capillaries absorb the excess leaked fluid (now called lymph) and any escaped proteins from the interstitial space. The lymphatic vessels carry this fluid through cleansing lymph nodes and eventually dump it back into the venous bloodstream near the heart (via the subclavian veins), perfectly maintaining overall blood volume.
Part 9: Special Circulations (Hepatic & Fetal)
9.1 The Hepatic Portal System
A "portal system" is a highly unique vascular arrangement where blood flows through two consecutive capillary beds before returning to the heart. The hepatic portal system connects the digestive organs to the liver.
The Hepatic Portal System Anatomy
Physiological Purpose:
Veins draining the stomach, intestines, spleen, and pancreas do not simply dump their blood into the inferior vena cava. Instead, they merge to form the Hepatic Portal Vein, which carries this blood directly to the liver.
This blood is rich in newly absorbed nutrients, but also potentially laden with toxins, bacteria, or alcohol. The liver's massive sinusoidal capillaries allow hepatic macrophages to cleanse the blood of bacteria, and hepatocytes to process nutrients and detoxify poisons before this blood is allowed to enter the general systemic circulation.
9.2 Fetal Circulation and Congenital Defects
Fetal circulation differs drastically from postnatal circulation because the fetal lungs are collapsed, fluid-filled, and completely non-functional for gas exchange. The fetus receives all oxygen and nutrients directly from the mother via the Placenta. Therefore, the fetal cardiovascular system possesses three unique vascular shunts to bypass the liver and lungs.
Fetal Circulation and Shunts
The Three Fetal Shunts:
Ductus Venosus (Bypassing the Liver): Fresh, highly oxygenated blood from the placenta travels up the umbilical vein. Most of this blood enters the ductus venosus, which shunts it straight into the Inferior Vena Cava, entirely bypassing the immature fetal liver capillary beds.
Foramen Ovale (Bypassing the Lungs): As blood enters the right atrium, it needs to avoid the non-functional lungs. The foramen ovale is a physical hole in the interatrial septum. Because pressure in the right heart is higher than the left heart in a fetus, most blood is blown straight through this hole from the Right Atrium directly into the Left Atrium, bypassing the right ventricle and pulmonary circuit.
Ductus Arteriosus (Bypassing the Lungs): The small amount of blood that does enter the right ventricle is pumped into the pulmonary trunk. However, the ductus arteriosus—a large vessel connecting the pulmonary trunk directly to the aorta—shunts this blood immediately into the systemic circulation, keeping it away from the high-resistance, fluid-filled lungs.
At birth, as the baby takes its first breath, lung resistance plummets, left heart pressure spikes, and these fetal shunts snap shut, permanently separating the pulmonary and systemic circuits. However, congenital defects can cause abnormal shunting after birth.
The Pathology of VSD:
The superior part of the interventricular septum fails to form completely, leaving a hole between the two ventricles.
Because the Left Ventricle has roughly three times the muscle mass and generates massively higher pressure than the right ventricle, blood is forcefully shunted from the Left Ventricle into the Right Ventricle during every systole. This is known as a Left-to-Right Shunt.
Consequently, already-oxygenated blood is uselessly pumped back into the pulmonary trunk, forcing the right ventricle and the lungs to handle a dangerous, massively increased volume of blood, eventually leading to right-sided heart failure.
Part 9.5: Lecture 5 Glossary (Cardiovascular System Terms)
Review this comprehensive glossary summarizing the essential anatomical and physiological terms discussed in this lecture before beginning the final confirmation questions.
Term (English)
Latin / Italian Counterpart
Physiological Role & Description
Epicardium
Epicardio (Italian)
The visceral layer of the serous pericardium, forming the thin outermost layer of the heart wall.
Myocardium
Miocardio (Italian)
The thick middle layer of the heart wall, composed of contracting cardiomyocytes and the fibrous skeleton.
Endocardium
Endocardio (Italian)
The thin inner lining of the heart chambers, consisting of a simple squamous endothelium resting on connective tissue.
PMI (Point of Maximal Intensity)
Itto della punta (Italian) / Apex beat
The location where the apex of the heart contacts the chest wall, typically in the 5th intercostal space along the left midclavicular line.
Trabeculae Carneae
Trabecole carnee (Italian)
Irregular muscular ridges lining the inner walls of the ventricular chambers.
Chordae Tendineae
Corde tendinee (Italian)
Collagenous cords anchoring the AV valve cusps to papillary muscles, preventing valve eversion during ventricular systole.
Systole & Diastole
Sistole e Diastole (Italian)
Systole refers to ventricular contraction and blood ejection; diastole refers to ventricular relaxation and chamber filling.
Functional Syncytium
Sincizio funzionale (Italian)
A network of cardiac muscle cells physically and electrically connected by gap junctions, allowing them to contract as a single unit.
Plateau Phase (Phase 2)
Fase di plateau (Italian)
The prolonged depolarization phase of cardiac action potentials, sustained by the balanced influx of calcium (L-type channels) and efflux of potassium.
Stroke Volume (SV)
Gittata sistolica (Italian)
The volume of blood pumped out of a ventricle per contraction, calculated as End-Diastolic Volume (EDV) minus End-Systolic Volume (ESV).
Cardiac Output (CO)
Gittata cardiaca (Italian)
The total volume of blood pumped by a ventricle per minute, calculated as HR × SV (normally ~5.25 L/min at rest).
Frank-Starling Law
Legge di Frank-Starling (Italian)
The biophysical principle stating that increased ventricular stretching (preload/EDV) increases the force of contraction, raising stroke volume.
Baroreceptors
Barocettori (Italian)
Stretch receptors located in the carotid sinuses and aortic arch that detect blood pressure fluctuations and signal the cardiovascular centers in the medulla.
RAAS Pathway
Sistema RAAS (Italian) / Renin-Angiotensin-Aldosterone System
Endocrine cascade initiated by low blood pressure; kidney renin converts angiotensinogen to AngI, which ACE converts to AngII, stimulating vasoconstriction and aldosterone release.
Starling Forces
Forze di Starling (Italian)
The hydrostatic and osmotic pressure gradients that govern fluid filtration and reabsorption across capillary walls.
Ductus Arteriosus
Dotto arterioso di Botallo (Italian)
A fetal vascular shunt connecting the pulmonary trunk directly to the aorta, bypassing non-functional lungs.
Part 10: The Ultimate IMAT Cardiovascular Simulator
This monumental 50-question examination rigorously tests every minute detail presented in this cardiovascular masterclass. The questions are explicitly designed at or above the grueling difficulty level of the official IMAT, focusing heavily on critical thinking, clinical applications, hemodynamics, and deep physiological mechanisms.