An exhaustive, university-level masterclass exploring Macroscopic Anatomy, Microscopic Histology of the Stomach & Intestines, Accessory Gland Architecture, and the Enteric Nervous System.
Est. Reading Time: 350 Mins 100% Curriculum Sync 50-Question Simulator
Human Digestive System Schematic
Digestive System Diagram
Gastrointestinal Motility
Lecture 1: Macroscopic Anatomy of the Gastrointestinal Tract
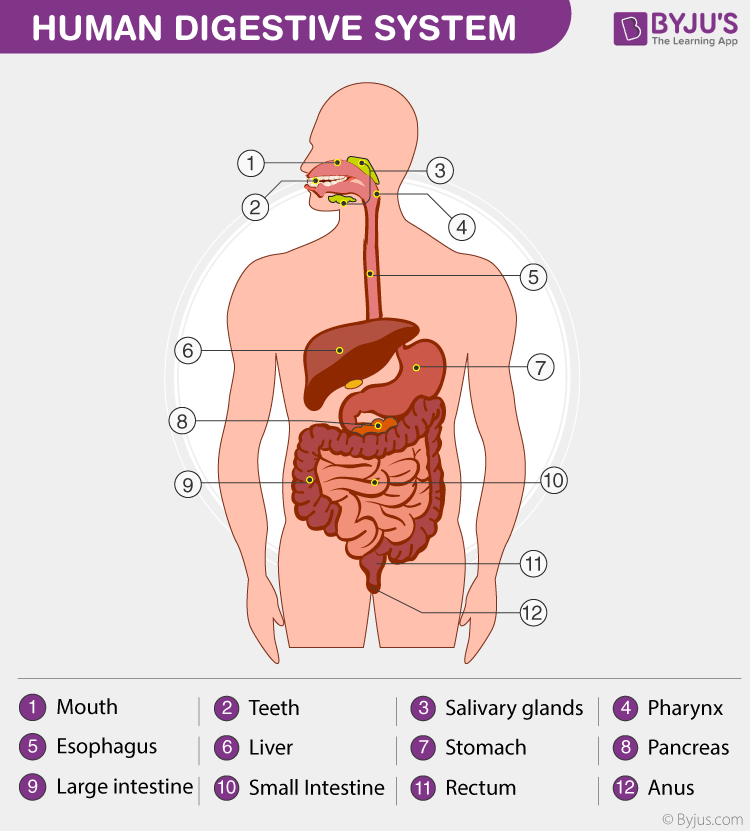
The digestive system is fundamentally a continuous muscular tube—the alimentary canal—extending from the oral cavity to the anus, functionally supported by numerous highly specialized accessory glands. Its primary mandate is to chemically and mechanically break down ingested macromolecules into absorbable monomers, extracting water, electrolytes, and nutrients, while subsequently compacting and eliminating indigestible waste.
Figure 1.1: Anatomical organization of the GI tract.
Stomach Architecture
Figure 1.2: Rugae and secretory regions of the stomach.
Small Intestine Surface
Figure 1.3: Microscopic villi for absorption.
1.1 Broad Anatomical Organization
From an anatomical standpoint, the digestive system is partitioned into two massive domains:
The continuous hollow passageway exposed to the external environment. It consists sequentially of:
Oral Cavity
Pharynx
Esophagus
Stomach
Small Intestine
Large Intestine
Rectum & Anal Canal
Accessory Glands & Organs
These structures lie entirely outside the alimentary canal but possess ducts that empty their vital enzymatic and emulsifying secretions directly into the lumen of the tract.
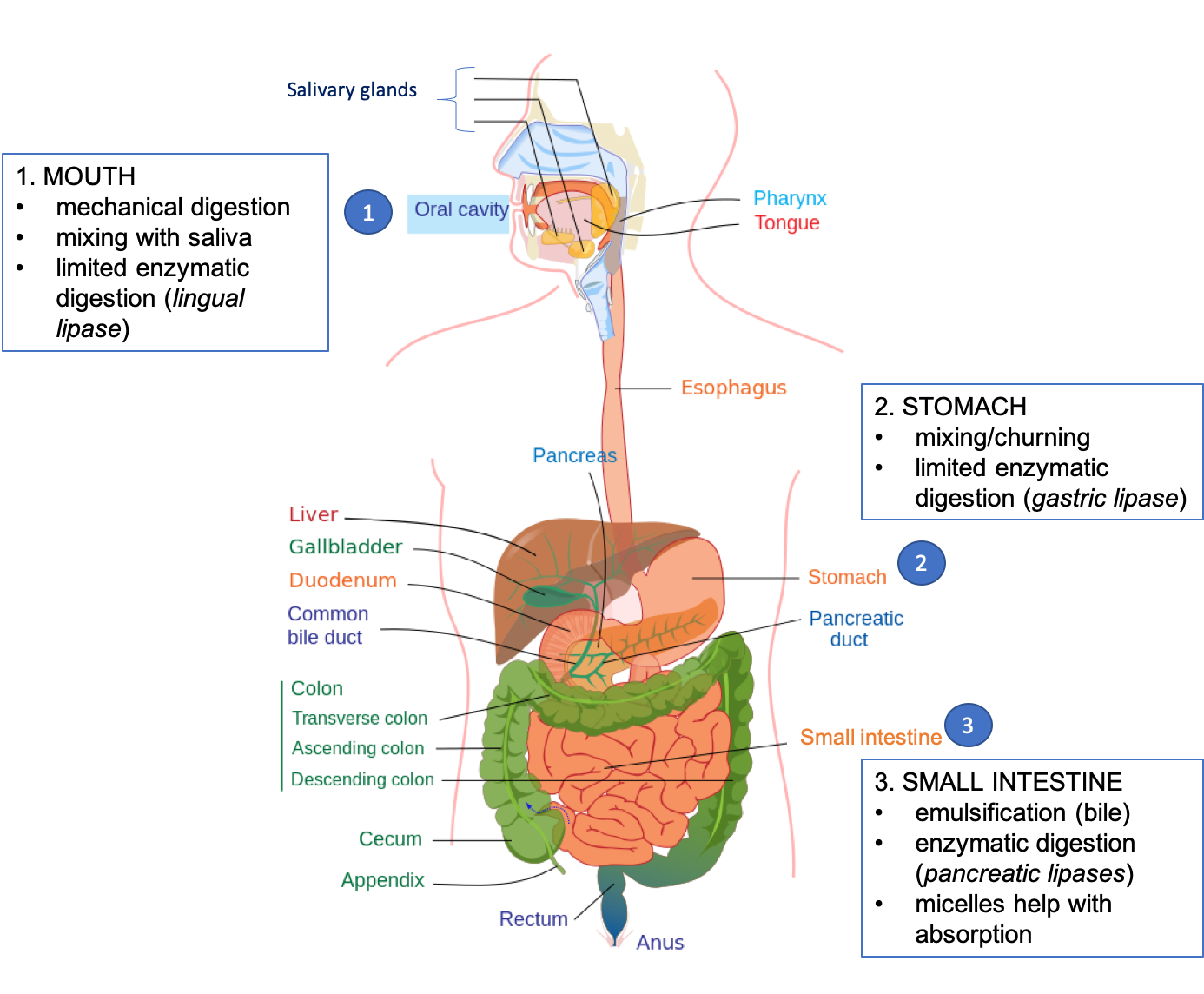
The journey begins in the oral cavity where mechanical digestion (mastication) and the initial stages of chemical digestion occur. The bolus is then propelled posteriorly into the Pharynx.
The Pharynx
The pharynx is a critical funnel-shaped muscular tube serving as a common crossroad for both the respiratory and digestive tracts. It is anatomically subdivided into three regions:
1. Nasopharynx
Posterior to the nasal cavity. Strictly an airway. Houses the pharyngeal tonsil and the opening of the auditory (Eustachian) tube.
2. Oropharynx
Posterior to the oral cavity. A shared passageway for both air and food/liquids. Houses the palatine and lingual tonsils.
3. Laryngopharynx
The most inferior portion. Diverges anteriorly into the larynx (guarded by the epiglottis) and posteriorly into the esophagus.
1.3 The Lower Alimentary Canal
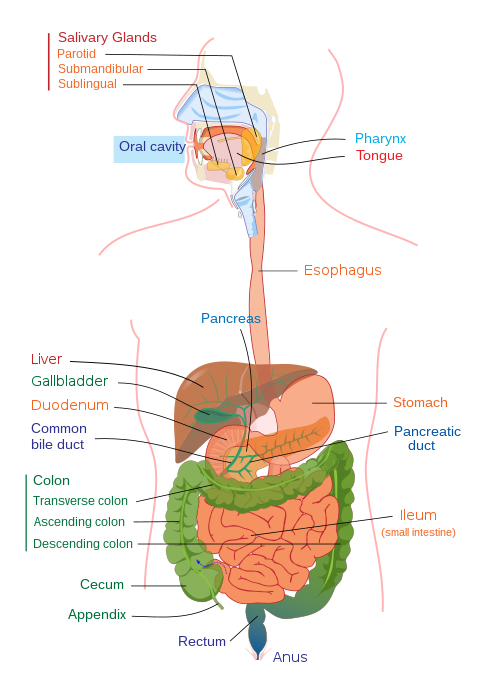
Figure 1.0: Macroscopic layout of the lower alimentary canal. Note the distinct transitions from the stomach to the small intestine (duodenum), and subsequently into the large intestine (colon).
The colon begins at the level of the ceco-colic orifice and continues to the rectum. It is heavily involved in the massive reabsorption of water and electrolytes, and the compaction of feces.
Ascending Colon
Transverse Colon
Descending Colon
Sigmoid Colon
Rectum & Anal Canal
The rectum increases in diameter and, at the level of the second/third coccygeal vertebra, forms a massive dilation known as the Rectal Ampulla.
The Dual Sphincters:
The terminal anal canal is strictly guarded by two sphincters: the Internal Anal Sphincter (composed of involuntary smooth muscle) and the External Anal Sphincter (composed of voluntary skeletal muscle).
Lecture 2: Microscopic Anatomy of the Stomach
Colon Symbiosis
Carbohydrate Digestion
Carbohydrate and Protein Digestion Pathway
Lipid Digestion Process
Lipid Digestion and Absorption
Digestive Anatomy NIDDK
Regulation of Blood Glucose
Zymogen Activation
Zymogen Activation Cascade
Hepatic Portal System
Liver Lobule
Liver Structure Cartoon
Sinusoids and Hepatocyte Co-transport
Liver Histology
Intestinal Villi
Villus Structure
Microvilli Molecular Transport
The stomach is a massive muscular sac acting as a food blender and reservoir. To withstand its own highly acidic and proteolytic secretions, the stomach wall possesses a complex, multi-layered histological architecture.
1. Tunica Mucosa
Extremely thick. Contains the gastric pits and deep gastric glands.
2. Tunica Submucosa
Dense connective tissue housing major blood vessels, lymphatics, and the submucosal nerve plexus.
3. Tunica MuscularisHighly unique! Possesses THREE layers of smooth muscle instead of the usual two:
Inner Oblique layer
Middle Circular layer
Outer Longitudinal layer
4. Tunica Serosa
The outermost protective layer of visceral peritoneum.
Microscopic Regions
Based purely on the type of glands present in the mucosa, the stomach is histologically divided into three regions: the narrow Cardiac region, the massive Fundic/Corpus region (oxyntic), and the Pyloric region.
2.2 Deep Dive: The Fundic (Oxyntic) Glands
The principal glands of the stomach are located in the fundus and the body (corpus). These deep, tubular glands are absolute chemical factories. They are lined by an incredibly diverse array of six distinct, highly specialized cell types.
Figure 2.0: The architectural layout of a typical Principal (Fundic) Gland, highlighting the intense stratification of highly specialized secretory cells along the depth of the gastric pit.
Cell Type
Histological Characteristics & Secretory Function
1. Surface Mucous Cells
Line the very surface and gastric pits. They secrete an incredibly thick, highly viscous, bicarbonate-rich mucus. This creates an impenetrable alkaline shield that absolutely protects the underlying stomach tissue from auto-digestion by its own harsh acid.
2. Mucous Neck Cells
Located down in the neck of the gland. They secrete a thinner, much more soluble, acidic mucus compared to the surface cells. Their exact physiological function is not fully understood, but it helps lubricate the gland lumen.
3. Parietal (Oxyntic) Cells
Massive, triangular cells concentrated in the middle of the gland. They are biological acid factories.
Hydrochloric Acid (HCl): Dropping the stomach pH to ~1.5. This extreme acidity sterilizes food, denatures proteins, and most importantly, physically activates pepsinogen into active pepsin.
Intrinsic Factor: A vital glycoprotein absolutely required for the absorption of Vitamin B12 in the terminal ileum. (Lack of this causes pernicious anemia).
5. Chief (Peptic) Cells
Located at the very base of the gland. They are packed with zymogen granules. They secrete Pepsinogen, a harmless, inactive proenzyme. Once secreted into the lumen, the brutal HCl from the parietal cells cleaves pepsinogen into Pepsin, a ruthless protein-digesting enzyme.
4. Neuroendocrine Cells
Scattered deep in the glands. They release chemical messengers directly into the interstitial fluid (not the lumen) to regulate digestion locally and systemically. Extremely difficult to observe in routine H&E sections. (e.g., G-cells releasing Gastrin).
6. Stem Cells
Undifferentiated, highly mitotic cells located in the isthmus/neck region. Because the stomach environment is so hostile, surface cells die rapidly. Stem cells continuously divide, migrating upward to replace surface cells (every 3-6 days) or migrating downward to differentiate into the deep glandular cells.
The Parietal Cell Acid Pump
The immense acidity of the stomach is driven by a specialized active transport pump on the apical membrane of the Parietal cell.
$$ H^+/K^+ \text{ ATPase (The Proton Pump)} $$
This pump burns massive amounts of ATP to force Hydrogen ions ($H^+$, protons) out into the stomach lumen against a million-fold concentration gradient, while simultaneously pulling Potassium ($K^+$) into the cell.
Pharmacology Note: Drugs like Omeprazole (Proton Pump Inhibitors) directly target and shut down this exact enzyme to treat severe acid reflux and ulcers.
Lecture 3: Microscopic Anatomy of the Intestines & Enteric Nervous System
The small intestine is the undisputed primary site of chemical digestion and massive nutrient absorption. To achieve this, its microscopic architecture is dedicated entirely to multiplying its internal surface area.
3.1 Intestinal Wall Architecture (Duodenum vs. Ileum)
The Duodenum
The first, shortest segment. It receives the highly acidic, dangerous chyme from the stomach.
Brunner's Glands
The absolute defining histological feature of the duodenum is the presence of massive, complex Brunner's Glands packed strictly within the Submucosa. These glands secrete copious amounts of highly alkaline, bicarbonate-rich mucus to instantly neutralize the incoming stomach acid, protecting the delicate intestinal walls.
The Ileum
The final, longest segment. Specialized for the absorption of Vitamin B12, bile salts, and remaining nutrients.
Peyer's Patches
The defining histological feature of the ileum is the presence of massive, aggregated lymphoid nodules called Peyer's Patches in the submucosa. Because the ileum is physically very close to the large intestine (which is packed with massive colonies of bacteria), these massive immune centers act as guardians, preventing bacteria from breaching the intestinal wall into the bloodstream.
To maximize absorption, the mucosa forms massive, finger-like projections called Villi extending into the lumen. The surface of these villi is lined with Simple Columnar Epithelium.
Enterocytes: The absorptive cells. Their apical surface is covered in microscopic Microvilli (the "brush border") which further multiply the surface area exponentially and contain final digestive enzymes.
Goblet Cells: Unicellular glands scattered among the enterocytes. They synthesize and secrete lubricating mucin to ease the passage of feces.
Paneth Cells: Located deep down in the intestinal crypts. They secrete antimicrobial agents (like defensins and lysozyme) to sterilize the crypts.
3.2 The Enteric Nervous System (The "Brain of the Gut")
The gastrointestinal tract possesses its own, incredibly sophisticated intrinsic nervous system. It contains over 100 million neurons (more than the entire spinal cord). It regulates motility (peristalsis) and glandular secretions completely autonomously, organized into two massive plexuses.
Figure 3.0: The exact histological location of the two massive neural networks that form the Enteric Nervous System.
1. Meissner's Plexus (Submucosal Plexus)
Location: Within the Submucosa.
Because it is located right beneath the mucosa, its primary role is to regulate the glandular secretions of the mucosa and to control the highly localized, fine movements of the Muscularis Mucosae (a tiny sliver of muscle in the mucosa that twitches the villi to enhance absorption).
2. Auerbach's Plexus (Myenteric Plexus)
Location: Sandwiched directly between the Inner Circular and Outer Longitudinal muscle layers of the Muscularis Externa.
Because it sits directly between the massive muscular driving engines of the tract, its primary, vital role is to control Gastrointestinal Motility. It orchestrates the massive, rhythmic waves of contraction known as Peristalsis and segmentation, crushing and propelling the food bolus forward.
Lecture 4: Accessory Glands - The Liver & Biliary System
The liver is the largest internal organ and the ultimate metabolic factory of the human body. Found in the upper right quadrant of the abdomen, it processes virtually every nutrient absorbed by the digestive tract, detoxifies the blood, and synthesizes Bile (crucial for fat emulsification).
4.1 Macroscopic Anatomy of the Liver
The liver is completely covered by the visceral peritoneum, with one profound exception: the Bare Area. This is a region on the superior-posterior aspect where the liver directly touches the diaphragm with no peritoneal covering.
Lobes and Ligaments
Right Lobe: Massive, dominates the right side.
Left Lobe: Smaller, extending to the left.
Falciform Ligament: A mesentery fold that physically separates the right and left lobes anteriorly and suspends the liver from the diaphragm and anterior abdominal wall.
Ligamentum Teres (Round Ligament): A fibrous cord running along the free edge of the falciform ligament. It is the anatomical remnant of the fetal umbilical vein.
Vascular Interactions
The liver is highly unique because it receives a dual blood supply. Highly oxygenated blood arrives via the Hepatic Artery. However, the majority of its blood volume arrives deoxygenated (but nutrient-rich) from the intestines via the Hepatic Portal Vein.
Hepatic Veins
After the liver's cells (hepatocytes) have cleansed the blood and processed the nutrients, the blood exits the liver via the Hepatic Veins, which dump immediately into the massive Inferior Vena Cava (IVC) lying on the liver's posterior surface.
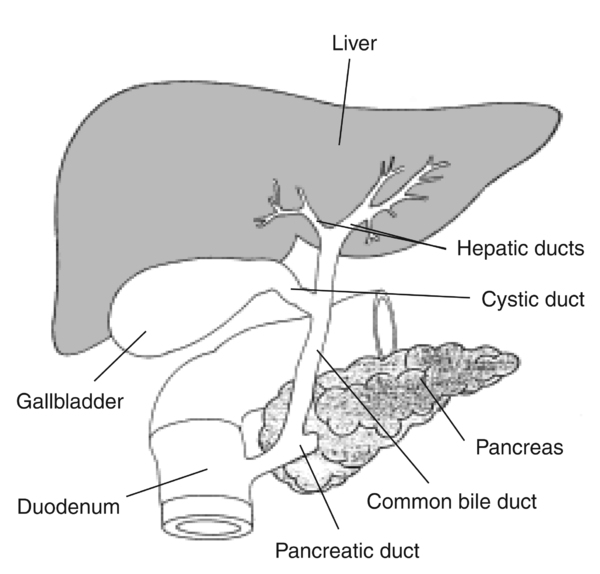
The Biliary Duct Pathway
Bile Pathway:
Hepatocytes produce bile $\rightarrow$ Right/Left Hepatic Ducts $\rightarrow$ Common Hepatic Duct.
Here it can either go to the Gallbladder for storage via the Cystic Duct, or it can merge to form the Common Bile Duct. The Common Bile Duct travels down to meet the main Pancreatic Duct, and they empty their powerful digestive fluids together into the Duodenum.
The functional unit of the liver is the hepatic lobule. It is a roughly hexagonal structure consisting of plates of hepatocytes radiating outward from a central vein, resembling a microscopic stop sign.
The Portal Triad
At each of the six corners of the hexagonal lobule sits a Portal Triad. It consists of three distinct vessels:
Branch of the Hepatic Artery: Supplying oxygen.
Branch of the Hepatic Portal Vein: Supplying nutrient-rich blood from the gut.
Bile Ductule: Collecting bile produced by hepatocytes and carrying it *away* from the center.
Blood from both the artery and the portal vein percolates through incredibly leaky capillaries called Liver Sinusoids towards the Central Vein. Inside these sinusoids lie hepatic macrophages (Kupffer cells) which brutally destroy incoming gut bacteria before they can reach the heart.
The pancreas is a massive, soft, tadpole-shaped gland located partially behind the stomach. It is highly unique because it is an Amphicrine gland (meaning it functions as both an exocrine and an endocrine gland simultaneously). It produces the digestive enzymes that break down all categories of foodstuff, making it the most vital chemical factory in digestion.
5.1 The Exocrine Pancreas (Digestive Juice)
The vast majority of the pancreas (approx. 99%) consists of exocrine tissue. It is histologically classified as a serous gland.
Figure 5.0: The structural unit of the Exocrine Pancreas. Note the defining presence of the Centroacinar Cell physically extending into the lumen of the acinus.
Acinar Cells
Pyramidal serous cells forming spherical clusters called Acini. They synthesize massive amounts of digestive enzymes.
The enzymes are stored securely inside the apical cytoplasm in dense spherical structures called Zymogen Granules to prevent the pancreas from digesting itself.
The Ductal System
Pancreatic acini are highly unique structurally. The initial duct (the Intercalated Duct) actually begins inside the lumen of the acinus.
The nuclei of these duct cells located inside the acinus are referred to as Centroacinar Cells. These duct cells are not passive pipes; they actively secrete massive amounts of bicarbonate-rich, watery fluid to neutralize stomach acid.
5.2 The Endocrine Pancreas (The Islets of Langerhans)
Scattered randomly like tiny islands among the vast sea of exocrine acini are millions of highly vascularized endocrine cell clusters called the Islets of Langerhans, accounting for only 1% to 2% of the total pancreatic mass.
Alpha ($\alpha$) Cells
Produce GLUCAGON.
Released during fasting states when blood glucose is critically LOW. It targets the liver to break down glycogen into glucose (glycogenolysis) and synthesize new glucose from amino acids (gluconeogenesis), raising blood sugar back to homeostatic levels.
Beta ($\beta$) Cells
Produce INSULIN.
Released after a meal when blood glucose is HIGH. It acts forcefully on all body cells (especially muscle and adipose) to insert GLUT transporters into the membrane, sweeping glucose out of the blood and into the cells for energy or storage as fat/glycogen. This drops blood sugar back to normal.
Delta ($\delta$) Cells
Produce SOMATOSTATIN.
The universal "off switch." It acts in a paracrine manner locally within the islet to heavily inhibit the secretion of both insulin and glucagon (particularly inhibiting the alpha cells), preventing extreme, dangerous hormonal swings.
膵臓の組織学(外分泌腺と内分泌部)/ Pancreas Histology Reference
消化酵素を生成する「腺房(Acini)」と、ホルモンを分泌する「ランゲルハンス島(Islets of Langerhans)」の対比図です。外分泌と内分泌の機能を区別して理解するのに役立ちます。
Lecture 6: The Comprehensive IMAT Digestive Database
For the IMAT examination, rote memorization of histology, cell types, specific organ secretions, and overall anatomical layout is completely non-negotiable. The following exhaustive table compiles the entirety of the digestive system covered in the masterclass into an ultra-high-yield, rapid-review format.
Organ / Structure
Histological Feature / Cell Type
Primary Secretion
Physiological Function
Pharynx
Nasopharynx, Oropharynx, Laryngopharynx
Mucus (Lubrication)
Common passageway for air and food bolus. Initiates swallowing reflex.
Stomach (Fundic Glands)
Surface Mucous Cells
Thick, Alkaline (Bicarbonate) Mucus
Protects stomach lining from auto-digestion by its own acid.
Mucous Neck Cells
Thin, Acidic Mucus
Lubricates the gland lumen.
Parietal (Oxyntic) Cells
HCl & Intrinsic Factor
HCl drops pH to ~1.5 to activate pepsinogen. Intrinsic Factor is absolutely required for Vitamin B12 absorption.
Chief (Peptic) Cells
Pepsinogen
Harmless proenzyme. Cleaved by HCl into active Pepsin to digest proteins.
Neuroendocrine Cells (e.g., G-Cells)
Gastrin, Histamine, Serotonin
Paracrine/Endocrine regulation of digestion. Gastrin heavily stimulates Parietal cells.
Stem Cells
N/A
Highly mitotic. Replace destroyed surface cells every 3-6 days.
Small Intestine
Duodenum: Brunner's Glands
Massive Alkaline Mucus
Located exclusively in submucosa. Instantly neutralizes acidic stomach chyme.
Ileum: Peyer's Patches
Lymphocytes / Antibodies
Aggregated lymphoid nodules in submucosa. Protects against bacteria from large intestine.
Enterocytes (Brush Border)
Brush Border Enzymes
Massive surface area for primary nutrient absorption.
Goblet Cells
Mucin
Lubricates passing chyme/feces.
Paneth Cells
Defensins, Lysozyme
Antimicrobial defense deep in intestinal crypts.
Enteric Nervous System
Meissner's Plexus
Neural Impulses
Located in Submucosa. Controls mucosal glandular secretions and Muscularis Mucosae micro-movements.
Auerbach's Plexus
Neural Impulses
Located in Muscularis Externa (between circular/longitudinal). Controls massive GI Motility (Peristalsis).
Liver
Hepatic Lobule (Hepatocytes)
Bile
Metabolic processing. Synthesizes Bile to physically emulsify fats in the duodenum.
Part 6.5: Lecture 8 Glossary (Digestive System Terms)
Review this comprehensive glossary summarizing the essential anatomical and physiological terms discussed in this lecture before beginning the final confirmation questions.
Term (English)
Latin / Italian Counterpart
Physiological Role & Description
Peristalsis
Peristalsi (Italian)
Alternating waves of smooth muscle contraction and relaxation that propel food unidirectionally along the gastrointestinal tract.
Segmentation
Segmentazione (Italian)
Non-propulsive contractions of circular smooth muscle that mix chyme with digestive secretions and bring it into contact with the mucosa for absorption.
Parietal Cells
Cellule parietali (Italian)
Gastric gland cells that secrete hydrochloric acid (HCl) to activate pepsinogen and kill pathogens, and intrinsic factor for Vitamin B12 absorption.
Chief Cells
Cellule principali (Italian)
Gastric gland cells that secrete inactive pepsinogen, which is converted to active pepsin in the acidic environment of the stomach lumen.
Pepsin
Pepsina (Italian)
The primary protein-digesting enzyme of the stomach, active in acidic pH, cleaving proteins into smaller peptides.
Brunner's Glands
Ghiandole di Brunner (Italian)
Glands located in the submucosa of the duodenum that secrete an alkaline, bicarbonate-rich mucus to neutralize acidic gastric chyme.
Peyer's Patches
Placche di Peyer (Italian)
Aggregated lymphoid follicles located in the mucosa/submucosa of the ileum, preventing bacterial overgrowth and providing mucosal immunity.
Enterocytes
Enterociti (Italian)
Columnar absorptive cells lining the small intestine, featuring microvilli (brush border) containing digestive enzymes.
Paneth Cells
Cellule di Paneth (Italian)
Specialized secretory cells at the base of intestinal crypts that release antimicrobial agents like lysozymes and defensins.
Bile
Bile (Italian)
An alkaline fluid produced by hepatocytes, containing bile salts that emulsify fats to increase surface area for pancreatic lipase.
Hepatic Portal Vein
Vena porta (Italian)
The major blood vessel carrying nutrient-rich, deoxygenated blood from the gastrointestinal tract directly to the liver sinusoids.
Centroacinar Cells
Cellule centroacinose (Italian)
Cells at the beginning of pancreatic intercalated ducts that secrete bicarbonate ions to neutralize duodenal acid under secretin stimulation.
Meissner's Plexus
Plesso di Meissner (Italian)
Part of the enteric nervous system located in the submucosa, regulating glandular secretions, local blood flow, and mucosal folding.
Auerbach's Plexus
Plesso di Auerbach (Italian)
Part of the enteric nervous system located between the circular and longitudinal muscle layers, regulating GI motility.
Part 7: The IMAT Digestive Simulator
This massive, comprehensive 50-question examination rigorously tests the exhaustive details presented in all preceding lectures of this masterclass. Designed strictly at the official IMAT difficulty level, it focuses heavily on histological differentiation, biochemical cellular mechanics, clinical deduction, and exact anatomical landmarks. Do not begin until you have absolutely mastered the material above.