Meditaliano IMAT Preparation
Lesson 20: Immunity and Homeostasis
Introduction: Defense and Balance
This comprehensive guide covers the two pillars of physiological stability: Immunity (how we defend against pathogens) and Homeostasis (how we maintain internal balance). Mastering these complex feedback loops and cellular interactions is crucial for the IMAT, as they form the foundation of human physiology and pathology.
0. Pathogens & Evolution
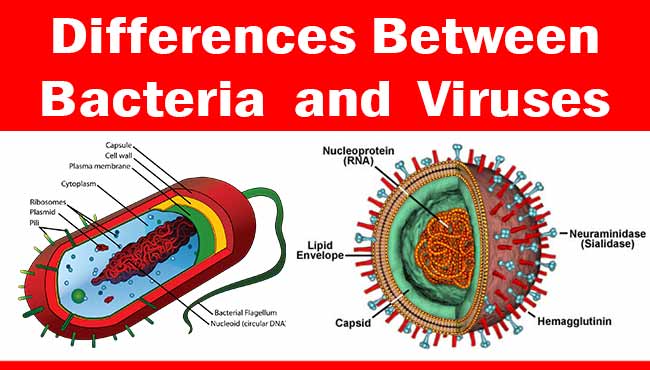
Before diving into how our immune system fights off invaders, it is essential to understand the structure of the most common pathogens. A pathogen is any organism that can produce disease. They range from microscopic viruses to large macroscopic parasites.
- Viruses: Non-living infectious agents consisting merely of genetic material (DNA or RNA) enclosed in a protein coat (capsid). They require a host cell machinery to replicate.
- Bacteria: Living, single-celled prokaryotes capable of independent reproduction. They have cell walls containing peptidoglycan.
- Fungi: Eukaryotic organisms (like yeast or mold) with cell walls made of chitin. Often cause opportunistic infections.
- Parasites: Eukaryotic organisms ranging from single-celled protozoa (e.g., Plasmodium causing Malaria) to multicellular helminths (worms).

Because bacteria are living organisms, they can be treated with antibiotics. However, overuse or misuse of antibiotics leads to immense evolutionary pressure.

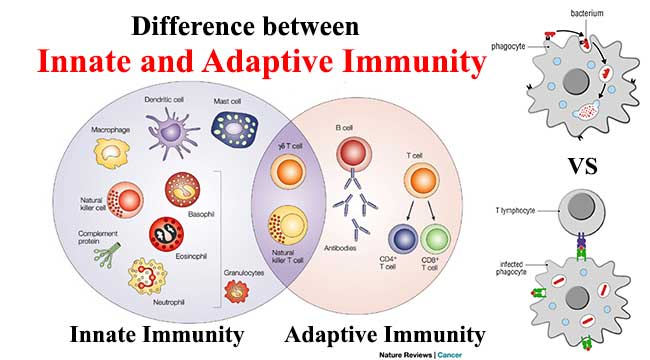
Part 1: Innate Immunity (Non-Specific)
The Innate Immune System is the first line of defense. It is immediate, non-specific (reacts to broad categories of pathogens), and lacks immunological memory.
1.1 Physical & Chemical Barriers
- Skin: A tough, keratinized physical barrier. Sweat and sebum create a low pH environment (Acid Mantle) that inhibits bacterial growth.
- Mucous Membranes: Lines respiratory, digestive, urinary, and reproductive tracts. Mucus traps pathogens; cilia in the respiratory tract sweep them out (Mucociliary escalator).
- Lysozyme: An enzyme found in tears, saliva, breast milk, and sweat that attacks the peptidoglycan cell walls of Gram-positive bacteria.
- Stomach Acid: Low pH (HCl, pH ~2) destroys most ingested pathogens and denatures their proteins.
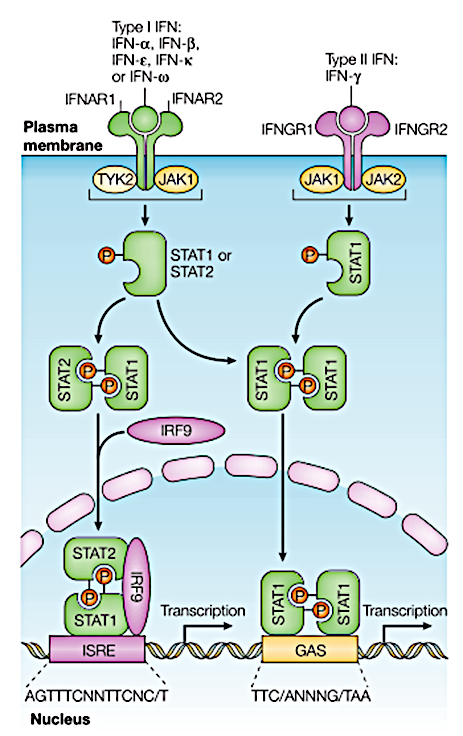
- Interferons: Anti-viral proteins secreted by virus-infected cells.
1.2 Phagocytosis & Pattern Recognition
When pathogens breach the physical barriers, phagocytic cells (Neutrophils, Macrophages, and Dendritic cells) recognize them using specialized receptors called Toll-like Receptors (TLRs). TLRs bind to Pathogen-Associated Molecular Patterns (PAMPs), such as bacterial lipopolysaccharide (LPS) or viral double-stranded RNA.
Diagram: The Process of Phagocytosis

1.3 Natural Killer (NK) Cells
While macrophages engulf extracellular pathogens, what happens to viruses hiding inside our own cells? Natural Killer (NK) cells are innate lymphocytes that patrol the body looking for abnormal host cells (virus-infected cells or cancer cells). They recognize cells that have down-regulated their MHC Class I molecules and release perforins and granzymes to induce apoptosis (programmed cell death) in the target cell.
1.4 Inflammation & Complement
When tissues are damaged, the body triggers an inflammatory response to isolate the infection and recruit immune cells.

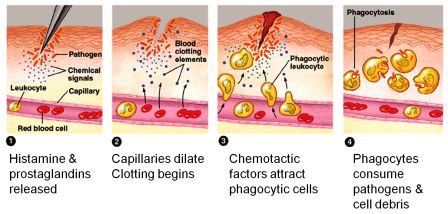
- Inflammation: The classic signs are Rubor (redness), Calor (heat), Tumor (swelling), and Dolor (pain). Driven largely by Histamine from Mast cells and Basophils.
- Complement System: A cascade of ~30 plasma proteins (C1-C9) synthesized by the liver that circulate in an inactive form. When activated, they:
- Opsonization: Coat pathogens (like a tag) to massively enhance phagocytosis.
- Chemotaxis: Attract more macrophages and neutrophils.
- MAC (Membrane Attack Complex): Punches physical holes in bacterial membranes, causing osmotic lysis.
1.5 The Lymphatic System
The lymphatic system is the battleground where innate immunity meets adaptive immunity. It collects excess interstitial fluid (lymph) and screens it for foreign antigens before returning it to the cardiovascular system.

Primary organs (Bone Marrow and Thymus) are where lymphocytes are produced, mature, and undergo negative selection (learning to tolerate "self" antigens).
Secondary organs (Lymph Nodes, Spleen, Tonsils, MALT/Peyer's Patches) are where mature, naive lymphocytes encounter antigens and are activated to mount immune responses. Source: ResearchGate

Part 2: Adaptive Immunity (Specific)
If the innate system is overwhelmed, the Adaptive Immune System kicks in. It is specific (targets exact molecular shapes called epitopes) and develops Immunological Memory.
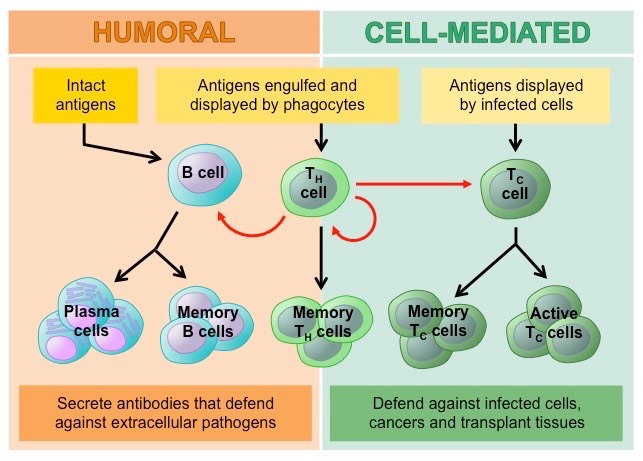
Humoral immunity involves B-cells producing antibodies to neutralize extracellular pathogens (viruses in the blood, bacteria, toxins).
Cell-mediated immunity involves Cytotoxic T-cells directly destroying infected or abnormal host cells. Helper T-cells act as the central command, releasing cytokines to stimulate both pathways. Source: bioninja.com.au
2.1 Lymphocytes & MHC Presentation
T-cells cannot recognize free-floating antigens. The antigen must be processed and "presented" on a special protein tray called the Major Histocompatibility Complex (MHC).
| Type | Origin / Maturation | Function & Activation |
|---|---|---|
| B-Cells | Bone Marrow / Bone Marrow | Humoral Immunity. Recognize intact, free antigens via BCR (IgD/IgM). Differentiate into Plasma Cells to secrete massive amounts of antibodies. |
| Helper T-Cells ($T_h$, CD4+) | Bone Marrow / Thymus | Commanders. Recognize processed antigens presented on MHC Class II. Secrete cytokines (e.g., Interleukin-2) to activate B-cells, Cytotoxic T-cells, and Macrophages. |
| Cytotoxic T-Cells ($T_c$, CD8+) | Bone Marrow / Thymus | Cell-Mediated Immunity. Recognize intracellular viral/tumor antigens presented on MHC Class I. Kill infected host cells directly via perforin and granzymes. |
To prevent accidental autoimmune attacks, lymphocytes require two signals to fully activate.
Signal 1: The specific antigen binding to the T-cell or B-cell receptor.
Signal 2: A co-stimulatory signal (e.g., CD28 binding to B7 on the APC, or cytokines from a Helper T-cell).
MHC Class I is found on ALL nucleated body cells. It presents endogenous (intracellular) antigens to CD8+ Cytotoxic T-cells. Think of it as a cell waving a flag saying, "I am infected, kill me!"
MHC Class II is found ONLY on professional Antigen Presenting Cells (APCs: Macrophages, Dendritic Cells, B-cells). It presents exogenous (extracellular) antigens to CD4+ Helper T-cells. Think of it as a scout showing the commander a picture of the enemy. Source: ResearchGate
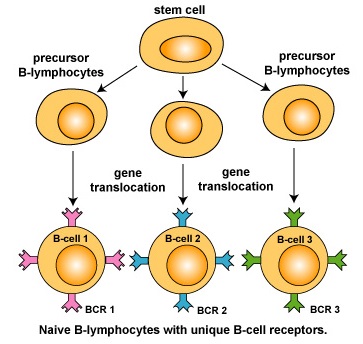
2.2 Clonal Selection Theory
How does the body produce exactly the right antibody out of millions of possibilities, even for synthetic molecules it has never seen before?

Part 3: Antibodies, Responses & Vaccines
3.1 Antibody Structure & Isotypes
Antibodies (Immunoglobulins, Ig) are quaternary proteins formed by 4 polypeptide chains. They do not kill pathogens directly; instead, they neutralize toxins, agglutinate pathogens, and tag them for destruction (opsonization) by macrophages or complement.
Diagram: Structure of an IgG Antibody
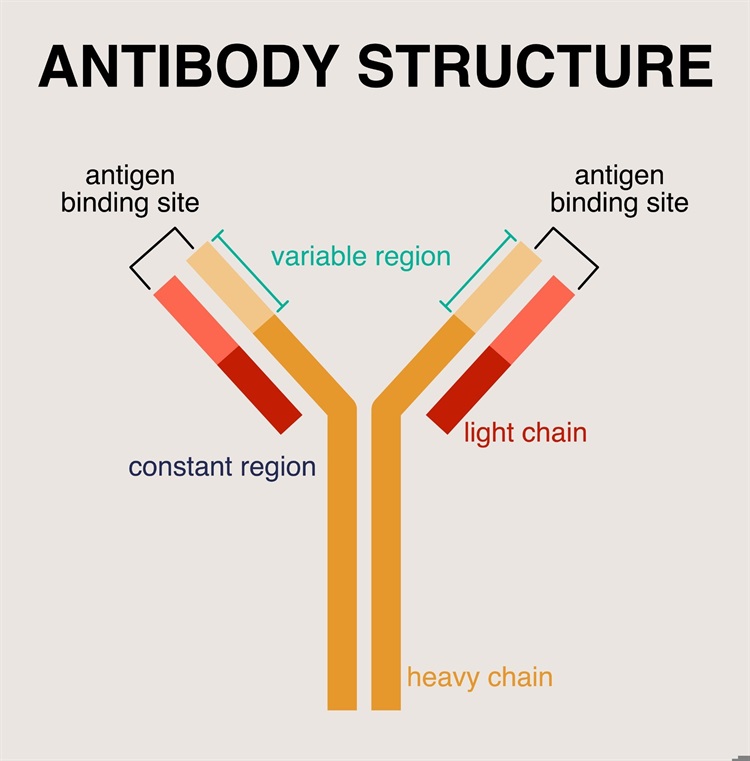
During an infection, an activated B-cell can undergo Class Switching. The variable region (target specificity) remains the exact same, but the constant Fc region is swapped to change the antibody's function (e.g., switching from IgM to IgG).
| Isotype | Description |
|---|---|
| IgG | Most abundant in blood/plasma (80%). The only antibody that can cross the placenta to provide passive immunity to the fetus. Indicator of long-term immunity. |
| IgM | Pentamer (5 structural units linked together). First antibody produced in a primary response. Highly effective at agglutination and complement activation due to its 10 binding sites. |
| IgA | Dimer. Found heavily in mucosal secretions (saliva, tears, respiratory mucus, breast milk). Provides localized protection on mucosal surfaces. |
| IgE | Binds to Fc receptors on Mast Cells and Basophils. Triggers histamine degranulation in Allergies and is essential for defending against parasitic worms. |
| IgD | Primarily functions as an antigen receptor on the surface of naive B-cells. |
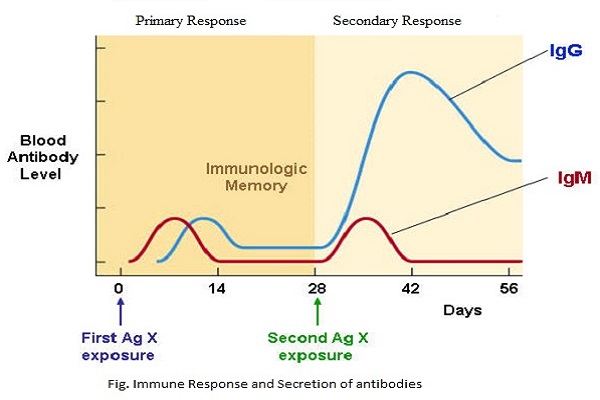
3.2 Primary vs. Secondary Response & Immunity Types
The secondary response is significantly faster, stronger, and longer-lasting due to the presence of Memory B and T cells generated during the first exposure.
1. Active Immunity: The body's own immune system generates antibodies and memory cells in response to an antigen. Takes time to develop but provides long-lasting protection.
Natural: Surviving a clinical infection.
Artificial: Vaccination (injecting harmless antigens/attenuated pathogens).
2. Passive Immunity: Pre-made antibodies are given to the individual. Provides immediate but temporary protection (no memory cells formed).
Natural: Maternal IgG crossing the placenta, or IgA in breast milk.
Artificial: Injecting antivenom or monoclonal antibodies (e.g., Rabies immunoglobulin).
3.3 Monoclonal Antibodies (Biotechnology)
Monoclonal antibodies (mAbs) are artificially produced antibodies that are identical and target a single specific epitope. They are extensively used in diagnostics (e.g., pregnancy tests using anti-hCG mAbs, COVID-19 rapid antigen tests) and therapeutics (e.g., targeted cancer therapies like Trastuzumab/Herceptin, or autoimmune suppressants).


Part 4: Immune Disorders & Blood Typing
4.1 Allergies (Hypersensitivity Type I)
An exaggerated, damaging immune response to normally harmless environmental antigens (allergens like pollen, peanuts).
4.2 Autoimmune & Immunodeficiency Diseases
- Autoimmune Diseases: The immune system fails negative selection, loses self-tolerance, and attacks the body's own tissues.
- Type 1 Diabetes: T-cells destroy pancreatic beta cells.
- Rheumatoid Arthritis: Inflammation and destruction of synovial joints.
- Multiple Sclerosis: T-cells attack the myelin sheath of central nervous system neurons.
- Immunodeficiency:
- SCID (Severe Combined Immunodeficiency): Genetic defect (often ADA deficiency) resulting in a total lack of functional B and T cells. Patients must live in sterile bubbles.
- AIDS (Acquired Immunodeficiency Syndrome): Caused by the HIV virus.

4.3 Blood Types & Transfusions
Blood types are determined by glycoprotein antigens on the surface of red blood cells. The immune system naturally produces antibodies against the antigens it does not possess. If incompatible blood is transfused, these antibodies cause massive agglutination (clumping) and hemolysis of the donated RBCs.
- Type A: Has A antigens. Produces Anti-B antibodies.
- Type B: Has B antigens. Produces Anti-A antibodies.
- Type AB: Has both A & B antigens. Produces NO antibodies. (Universal Acceptor: AB+)
- Type O: Has NO antigens. Produces both Anti-A and Anti-B antibodies. (Universal Donor: O-)
4.4 Hemolytic Disease of the Newborn (Rh Incompatibility)
This disorder occurs when the Rhesus (Rh/D) factor clashes between a mother and her developing fetus.

Part 2: Homeostasis & Regulation
Homeostasis is the maintenance of a relatively constant internal physiological environment (temperature, pH, glucose, water potential) despite external fluctuations. It is primarily controlled by the nervous and endocrine systems using Negative Feedback Loops.
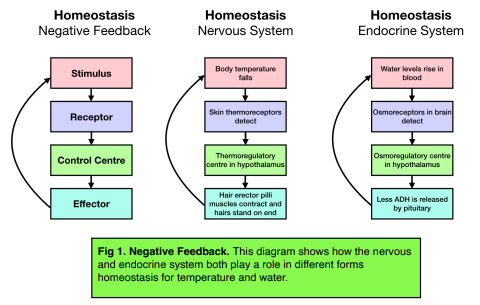
2.1 Thermoregulation
The control center for body temperature is the Hypothalamus. Set point: ~37°C. It monitors the temperature of the blood flowing through it and receives inputs from peripheral thermoreceptors in the skin.
Diagram: Thermoregulation Loop
- When Hot:
- Vasodilation: Arterioles supplying skin capillaries dilate. More warm blood flows near the surface, losing heat via radiation.
- Sweating: Sweat glands secrete water. As water evaporates, it absorbs a large amount of heat energy from the skin due to water's high latent heat of vaporization, cooling the body.
- When Cold:
- Vasoconstriction: Arterioles constrict, diverting blood away from the skin to internal organs to minimize heat loss.
- Shivering: Rapid, involuntary contraction of skeletal muscles generates heat as a byproduct of increased cellular respiration.
- Piloerection: Arrector pili muscles contract, raising hairs (goosebumps) to trap an insulating layer of still air (more effective in furry mammals than humans).

2.2 Blood Glucose Regulation & Diabetes
Maintaining a constant blood glucose concentration (~90mg/100ml) is vital, as the brain relies almost exclusively on glucose for ATP production. Controlled hormonally by the Islets of Langerhans in the Pancreas.
- High Glucose (After a meal): $\beta$-cells (Beta cells) detect the rise and secrete Insulin.
- Increases cellular uptake of glucose (by inserting GLUT4 transporters into muscle and fat cell membranes).
- Stimulates Liver and Muscles: Glucose $\rightarrow$ Glycogen (Glycogenesis).
- Increases lipid synthesis from excess glucose.
- Low Glucose (Fasting/Exercise): $\alpha$-cells (Alpha cells) detect the drop and secrete Glucagon.
- Stimulates Liver: Glycogen $\rightarrow$ Glucose (Glycogenolysis).
- Stimulates Liver: Amino acids/glycerol $\rightarrow$ Glucose (Gluconeogenesis).
- Note: During acute stress, the adrenal medulla releases Adrenaline (Epinephrine), which acts synergistically with glucagon to rapidly promote glycogenolysis for the "fight or flight" response.
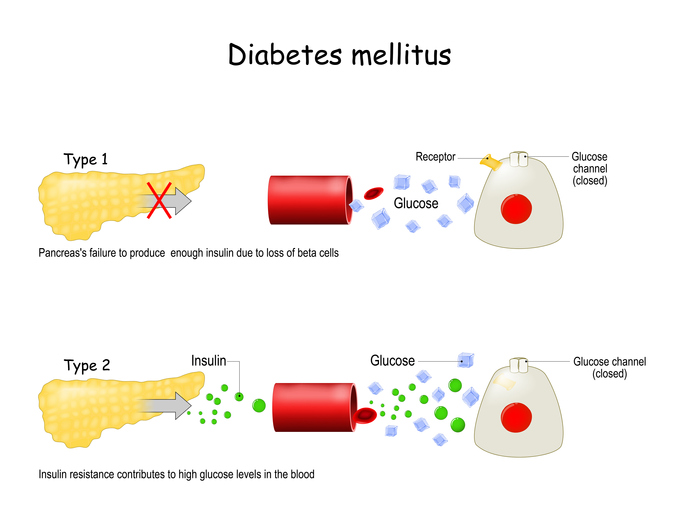
Type 1 (Juvenile onset): Autoimmune destruction of pancreatic beta cells results in an absolute lack of insulin. Requires insulin injections.
Type 2 (Adult onset): Associated with obesity and genetics. Target cells (muscle/liver) become resistant to insulin. The pancreas initially overworks to produce more insulin, but eventually fails to overcome this resistance. Source: painscale.com
2.3 Kidneys, Osmoregulation & BP
The kidneys filter blood to remove urea (nitrogenous waste) and carefully regulate the water and ion content of the blood. The functional unit of the kidney is the Nephron.
1. Ultrafiltration: High blood pressure in the Glomerulus forces water, glucose, ions, and urea into Bowman's capsule. Large proteins and RBCs remain in the blood.
2. Selective Reabsorption: In the Proximal Convoluted Tubule (PCT), 100% of glucose and most amino acids/ions are actively reabsorbed into the blood.
3. Loop of Henle: Creates a hypertonic (salty) medulla environment via a countercurrent multiplier system.
4. Collecting Duct: Variable water reabsorption based on ADH levels, determining the final urine concentration.
A. ADH (Antidiuretic Hormone) and Water Balance
Produced by the Hypothalamus, stored and released by the Posterior Pituitary. Released during Dehydration (High Osmolarity / Low water potential in blood).
- ADH binds to receptors on the Collecting Duct of the nephron.
- It causes aquaporins (water channels) to be inserted into the membrane.
- Water is drawn out of the collecting duct (by osmosis into the salty medulla) and reabsorbed into the blood.
- Result: Small volume of highly concentrated, dark urine. Blood osmolarity returns to normal.
Diagram: ADH Negative Feedback Loop
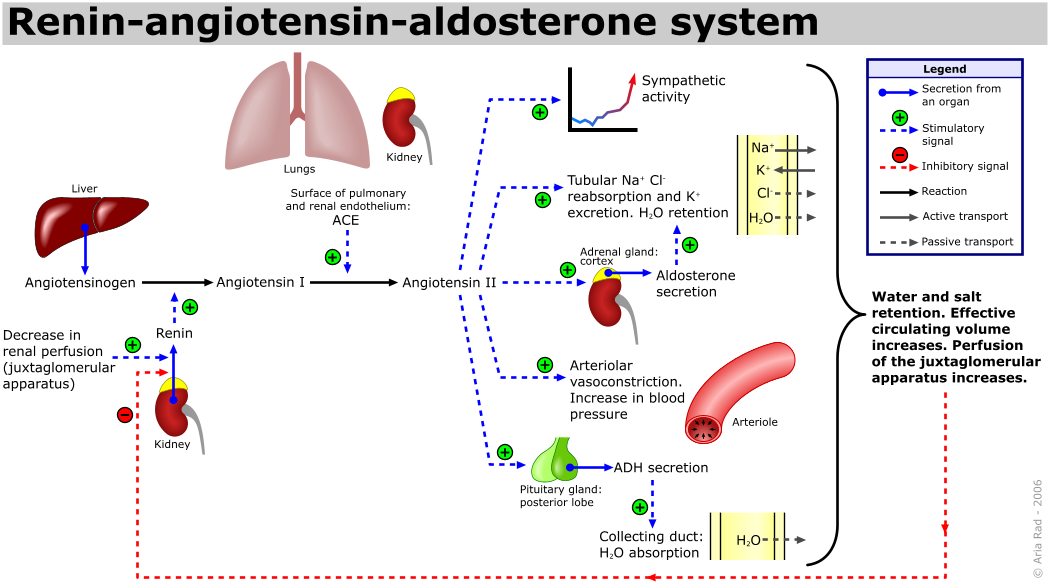
B. RAAS (Renin-Angiotensin-Aldosterone System)
Regulates Blood Volume and Blood Pressure. Triggered by a drop in blood pressure (e.g., hemorrhage) or low Na+ concentration detected by the kidney's juxtaglomerular apparatus.
2.4 Calcium Homeostasis
Calcium ($Ca^{2+}$) is essential for muscle contraction, nerve impulse transmission, and blood clotting. It is tightly regulated by two antagonistic hormones operating via negative feedback.
- Low Blood Calcium: The Parathyroid glands secrete Parathyroid Hormone (PTH).
- Stimulates osteoclasts to break down bone matrix, releasing Ca2+ into blood.
- Increases Ca2+ reabsorption in the kidneys.
- Activates Vitamin D to increase Ca2+ absorption in the intestines.
- High Blood Calcium: The Thyroid gland (C cells) secretes Calcitonin.
- Inhibits osteoclast activity and stimulates osteoblasts to deposit Ca2+ into bone.
- Increases Ca2+ excretion by the kidneys.

2.5 Positive Feedback
Unlike negative feedback which maintains stability, positive feedback amplifies the stimulus, moving the system further away from equilibrium. It is inherently unstable and is generally used for rapid, episodic events that must be driven to a definitive conclusion.
- Childbirth (Parturition): The head of the fetus pushes against the cervix. Stretch receptors send nerve impulses to the hypothalamus, triggering the posterior pituitary to release Oxytocin. Oxytocin causes stronger uterine muscle contractions, which pushes the baby harder against the cervix, causing more stretch and more Oxytocin release. This amplifying cycle continues until the climax (birth of the baby), which removes the initial stimulus.
- Blood Clotting (Coagulation Cascade): A damaged vessel exposes collagen. Platelets adhere and release chemical signals attracting more platelets, which release more signals. This cascade continues exponentially until the clot physically seals the break to stop bleeding.
- Action Potentials: In neurons, the opening of some voltage-gated Na+ channels depolarizes the membrane, which triggers the opening of more Na+ channels, leading to a rapid spike in membrane potential.
Comprehensive Practice Quiz
Test your knowledge on immunology and homeostasis. This quiz includes the newly added topics such as NK cells, blood types, and nephron physiology.